Zara Hayat ▫ BioBuilderClub, Andover High School, Andover, Massachusetts, United States
Reviewed on 6 May 2023; Accepted on 13 July 2023; Published on 16 October 2023
With help from the 2023 BioTreks Production Team.
Chimeric antigen receptor (CAR) T cell therapy has emerged as a promising immunotherapeutic approach for cancer treatment, harnessing the power of a patient’s own immune system. Despite significant advancements, traditional CAR T cell therapy faces challenges related to efficacy, persistence, and safety. Additionally, this method has shown immense difficulty in addressing the solid tumor microenvironment. Due to their substantial biocompatibility and unique properties which allow for a diverse range of compositions, nanoparticles (NPs) have served as a promising material for various biomedical and drug delivery applications. Previous research regarding NPs as a tool for targeted chemotherapy delivery has demonstrated an increase in therapeutic effects. They can be contained within a specific area of malignancy without spreading to the rest of the body, and due to their extremely small size, they have the ability to bypass the solid tumor microenvironment. Through the insertion of the CAR plasmid, nanoparticles can be harnessed to modify T cells within the body to bring about disease remission and therapy for solid tumor cancerous cells that are prone to develop recurrent mutations. CAR-carrying NPs represent a promising advancement in T cell therapy, offering distinct advantages over traditional CAR T cell therapy. Their ability to target multiple antigens, control CAR expression, and overcome immunosuppression makes them a compelling platform for next-generation CAR T cell therapy.
Keywords: Nanoparticles, T cell therapy, gene delivery, chimeric antigen receptor
Authors are listed in alphabetical order. Lindsey L’Ecuyer from BioBuilderClub, Andover High School, Andover, Massachusetts, United States mentored the group. Please direct all correspondence to .

T cells, also known as T lymphocytes, are a type of white blood cell that play a critical role in the immune system. They are a key component of the adaptive immune response, which is the body’s specific defense mechanism against pathogens like viruses, bacteria, and fungi (Cleveland Clinic, 2023). CAR (chimeric antigen receptor) T cell therapy is a type of immunotherapy that uses genetically modified T cells to treat cancer. CAR is a synthetic receptor that is engineered to recognize specific molecules, called antigens, on cancer cells. In this therapy, T cells are extracted from a patient’s blood and modified in a laboratory to express a CAR on their surface. The CAR is designed to recognize a specific antigen on the surface of cancer cells, such as CD22 in the case of solid tumors. Once the T cells have been modified to express the CAR, they are expanded in the laboratory to create a large population of CAR T cells. These CAR T cells are then infused back into the patient, where they can recognize and attack cancer cells that express the targeted antigen. When the CAR T cells encounter cancer cells, the CAR binds to the antigen on the cancer cell surface and activates the T cell to kill the cancer cell. The activated T cells then multiply and continue to attack the cancer cells, leading to tumor cell death (National Cancer Institute, 2022).
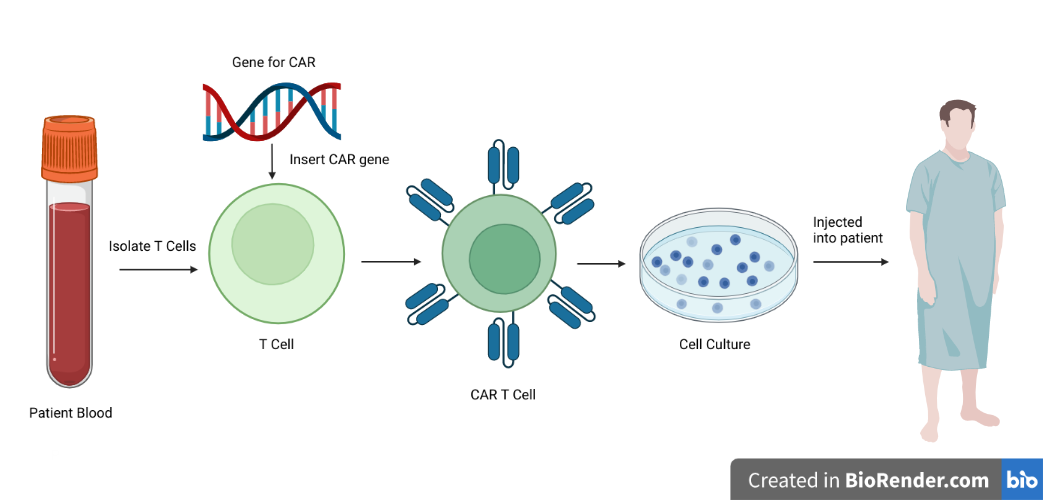
| Figure 1. Description of current CAR T cell method. T cells are isolated from the patients blood, CAR genes are inserted then grown in cell culture to be reinjected into the patient (Albinger & Hartmann, 2021). |
|---|
These methods have shown immense success in the application of hematological malignancies, such as acute lymphoblastic leukemia, multiple myeloma, chronic lymphocytic leukemia, and acute myeloid leukemia (Abbasi et al., 2022). Hematological malignancies are typically characterized by the expression of one specific antigen on the surface of cancer cells. For example, CD19 is a common antigen expressed on the surface of B-cell leukemia and lymphoma cells, where the CAR T cells are engineered to recognize CD19. As the therapy is able to leverage the unique properties of T cells, those of which are naturally programmed to recognize and attack specific targets, it enhances its specificity (Abbasi et al., 2022). Additionally, it is important to note that hematological cancer cells are not constricted by a microenvironment barrier that would restrict the T cell’s ability to reach it.
While CAR T cell therapy has shown promising results in clinical trials for hematological malignancies in immunostimulatory and immunosuppressive applications (Est-Witte et al., 2021), it can also cause side effects, including cytokine release syndrome and neurotoxicity. Cytokine release syndrome is a systemic inflammatory response that can cause fever, low blood pressure, and other symptoms, while neurotoxicity can cause confusion, seizures, and other neurological symptoms. Additionally, the complex manufacturing process of current autologous CAR T cells has infringed on its broader applications (Xin et al., 2022). Forms of T cell-based therapy in the clinic, such as adoptive cell transfer and vaccines are limited by cost, treatment times, and patient commitments (Est-Witte et al., 2021).
Finally, current CAR T cell therapy methods have proven ineffective in addressing the solid tumor microenvironment, which can create an immunosuppressive environment that hinders the activity of CAR T cells. The tumor microenvironment is a complex mixture of cells, extracellular matrix, and soluble factors that are present within and around the tumor. It includes immune cells, such as regulatory T cells and myeloid-derived suppressor cells, as well as stromal cells and extracellular matrix components, which can limit T cell infiltration and activity within the tumor (Zhang et al., 2022). One of the main challenges of CAR T cell therapy in solid tumors is the inability of CAR T cells to infiltrate the tumor and interact with cancer cells. In many solid tumors, the extracellular matrix can act as a physical barrier that prevents T cells from reaching the tumor cells. Additionally, the immunosuppressive nature of the tumor microenvironment can inhibit T cell activity and function, reducing the effectiveness of CAR T cell therapy (Zhang et al., 2022). Another challenge of CAR T cell therapy in solid tumors is the heterogeneity of antigen expression in cancer cells. Unlike hematological malignancies, which often express a single antigen that can be targeted by CAR T cells, solid tumors can express a variety of different antigens, or may have low or heterogeneous antigen expression, making it difficult for CAR T cells to selectively target cancer cells (Zhang et al, 2022).
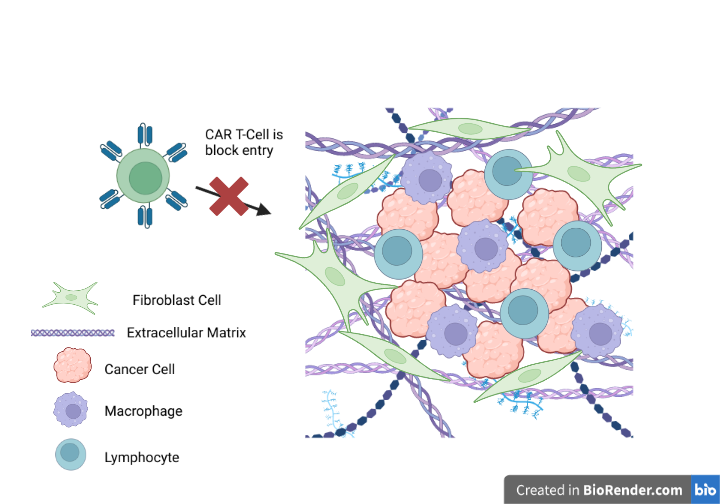
| Figure 2. Traditional CAR T cell entry into the solid tumor microenvironment is blocked. (Hou et al., 2021) |
|---|
Therefore, the interest in alternative nanotechnologies as methods to combat these difficulties has become apparent. NPs are materials with a dimension in the nanoscale, ideally under 100 nm. The use of nanotechnologies in CAR T cell therapy has the potential to improve the effectiveness and specificity of the therapy, overcome some of the challenges associated with solid tumors, and reduce off-target effects. Ongoing research is exploring the use of nanotechnology in combination with CAR T cell therapy to enhance the therapeutic potential of this promising approach to cancer treatment (Balakrishnan & Sweeney, 2021), as the development of NPs has been able to counteract the lack of specificity. Clinical applications of these engineered particles have been essential for targeted drug and gene delivery, usually through surface modification (Cao et al., 2020).
NPs in specific, offer a modular, universal platform to improve the efficacy of various T cell therapies as nanoparticle properties can be easily modified for enhanced cell targeting, organ targeting, and cell internalization (Est-Witte et al., 2021). Additionally, due to their high surface area to volume ratio, they often evade the immune system and circulate in the bloodstream with optimal patterns of drug delivery. NPs are too small to be detected by immune cells, such as macrophages, that would normally clear foreign particles from the body. NPs can be designed to be biodegradable, meaning that they can be broken down into smaller, non-toxic components by natural processes in the body. This is an important property for drug delivery, as it can reduce the risk of toxicity and other side effects associated with the accumulation of NPs in the body. Biodegradable NPs can be made from a variety of materials, such as lipids, proteins, and polysaccharides, which are metabolized and eliminated by the body over time (Abbasi et al., 2022). In comparison, current CAR T cell methods can end up harming healthy tissue if they are in the body too long because there is no system of degradation.
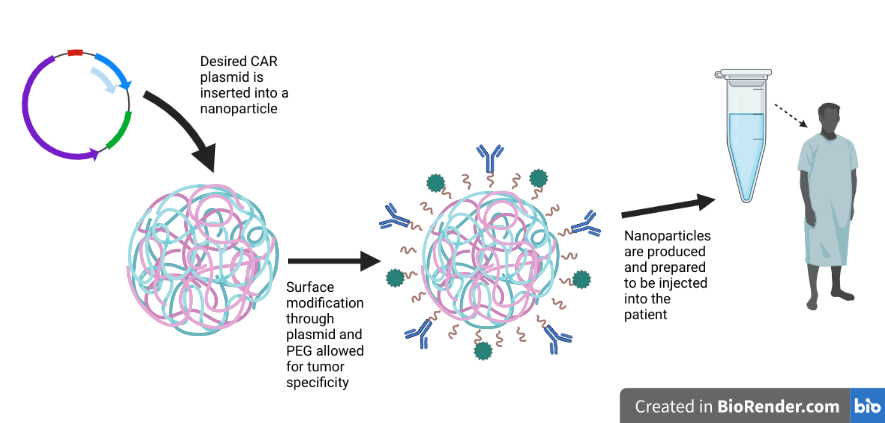
| Figure 3. Process by which CAR carrying NP is prepared to be injected into a patient |
|---|
Systems level
Current CAR T cell therapies represent engineered autologous T cells that express a synthetic CAR, which targets tumor associated antigens. These cells are made by harvesting T cells from the respective patient and reengineering them in vitro to produce the CAR protein on their surface (National Cancer Institute, 2022). Once T cells have been isolated, they are genetically modified to express a CAR. CARs are engineered receptors that combine the antigen-binding domain of an antibody with T cell signaling domains to allow T cells to recognize and kill cancer cells in a targeted manner (Xin et al., 2022). The process of genetic modification typically involves the use of a viral vector, such as a lentivirus or retrovirus, to deliver the CAR gene into the T cells. The viral vector integrates the CAR gene into the T cell genome, allowing the T cells to express the CAR protein on their surface.
After genetic modification, the CAR T cells are expanded in culture to generate a large number of cells for infusion. The expansion process typically involves the use of cytokines, such as IL-2 or IL-7, which stimulate T cell proliferation and survival. Each CAR acts as a cell membrane bridge. Both within and outside of the cell are portions of the receptor. The portion of the CAR that protrudes from the surface of the cell is often made up of pieces, or domains, of synthetic antibodies. How successfully the receptor identifies or binds to the antigen on tumor cells depends on which domains are used. Each CAR includes signaling and “co-stimulatory” domains within. Following an interaction between the receptor and an antigen, a signal cascade is initiated within the cell. The domains utilized can impact how well the cells work collectively (National Cancer Institute, 2022). Afterwards, the cells are mass produced to be infused back into the patient, where they will continue to multiply in the patient’s body and can travel to the site of the cancer and begin to recognize malignant cells.
However, these methods prove ineffective when considering the solid tumor microenvironment. This is where the improvement regarding DNA-carrying NPs becomes necessary. Instead of having extraneous T cell agriculture, the NPs will be infused with a plasmid containing the CAR genes. The surface of the NPs will be designed for specificity for certain T cells, allowing the NPs to deliver the CAR genes triggering the genetic transformation.
The first step in the process is to insert the CAR genes into the NP via a plasmid. Plasmids are small, circular pieces of DNA that are commonly used in genetic engineering to deliver genes into cells. The CAR genes are inserted into the plasmid, which is then loaded into the NP. The plasmid that will be used is 194-1BBz CAR, which is a fusion receptor composed of a single-chain antibody (scFv) specific for the extracellular domain of the antigen, combined with 4-1BB and CD3ζ cytoplasmic signaling domains. (Smith et al., 2017)
Once the NP is loaded with the CAR plasmid, it can be infused into the bloodstream.
As seen in Figure 4, the NPs are designed to circulate in the bloodstream and locate T cells. The NPs surface coating allows them to bind specifically to T cells, enabling targeted delivery of the CAR genes. When the NP reaches a T cell, it is taken up by the cell through a process called endocytosis. Once inside the T cell, the plasmid carrying the CAR genes is released from the NP and enters the nucleus of the cell. The CAR genes are then incorporated into the T cell genome, enabling the T cell to express the CAR protein on its surface. The expression of the CAR protein on the T cell surface enables it to recognize and bind specifically to a protein on the surface of the cancer cells, triggering the T cell to kill the cancer cells. This targeted approach minimizes damage to healthy cells and tissues, reducing potential side effects associated with traditional cancer treatments (Zhang, 2022).
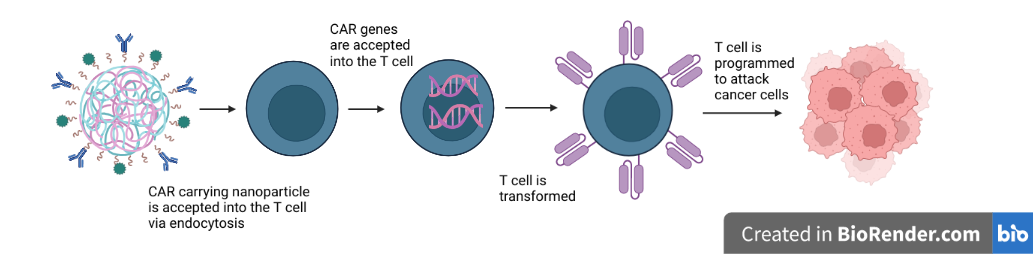
| Figure 4. In vivo transformation of T cells to attack cancer cells through the CAR carrying NP |
|---|
Device level
The main components of this system are the novel CAR technology, PEGylation coating, and nonviral vector approach. The 194-1BBz CAR plasmid is a key component of CAR T cell therapy. It contains the genetic sequence that codes for the CAR that is expressed on the surface of T cells, enabling them to recognize and attack cancer cells. The 194-1BBz CAR plasmid is constructed using recombinant DNA technology. The plasmid contains the genetic sequence for the CAR protein, as well as other regulatory sequences that control its expression (Smith et al., 2017).
Once the plasmid is constructed, it is then loaded into a NP complex for delivery into T cells. The NP complex is typically composed of a biodegradable polymer, such as poly(lactic-co-glycolic acid) (PLGA), that can encapsulate the plasmid and protect it from degradation in the bloodstream. To form the NP complex, the 194-1BBz CAR plasmid is mixed with the PLGA polymer in a solution. The solution is then subjected to a process called sonication, which uses sound waves to create NPs from the PLGA polymer. The resulting NPs have a diameter of approximately 100 nanometers and are able to encapsulate the 194-1BBz CAR plasmid (Shin et al., 2023). The 194-1BBz CAR plasmid and NP complex is then ready for delivery into T cells. The complex is typically infused into the bloodstream of the patient, where it circulates until it reaches the T cells.
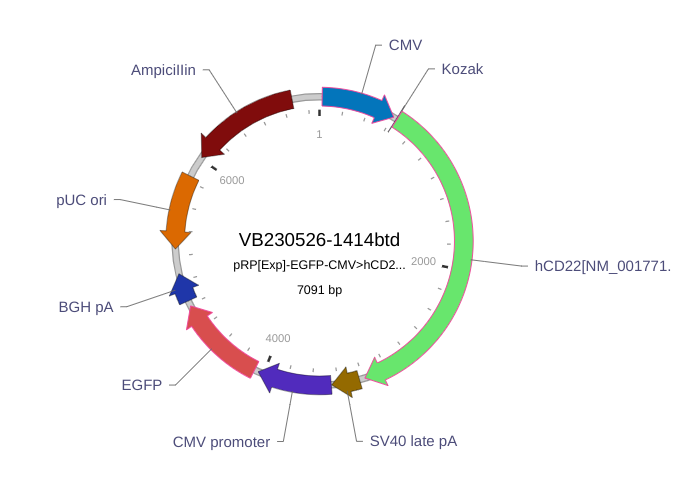
| Figure 5. Plasmid Map of anti-CD22 CAR (Atsavapranee et al., 2021) |
|---|
Once inside the T cell, the 194-1BBz CAR plasmid is able to integrate into the genome of the cell, enabling the T cell to express the CAR protein on its surface. The expression of the CAR protein enables the T cell to recognize and attack cancer cells, leading to the destruction of tumor cells and the reduction of relapsed cancerous growth.
Parts level
Current CAR T cell therapy often uses viral vectors to deliver the genetic material encoding the CAR into T cells. These viruses are modified to remove their ability to cause disease, while still maintaining their ability to efficiently deliver genes into cells. Transduction delivers the CAR gene via viral vectors into the T cells, resulting in a high percentage of T cells expressing the CAR on their surface. One major limitation is the potential for immune responses against the viral vector itself. Even when modified to reduce their ability to cause disease, viral vectors can still elicit an immune response, which can reduce the effectiveness of the therapy and even cause harm to the patient (Lukjanov et al., 2021). Another limitation of viral vector-based delivery is that the efficiency of gene transfer can vary depending on the type of virus and the cell type being targeted. For example, lentiviruses are more efficient at transducing T cells than retroviruses, but the efficiency of both viruses can be affected by the differentiation state of the T cells (Ramamoorth & Narvekar, 2015).
One of the main advantages of non-viral vectors is that they are generally safer and less immunogenic than viral vectors. Because they do not contain viral proteins or genetic material, they are less likely to trigger an immune response, reducing the risk of adverse effects. In addition, the manufacturing process for non-viral vectors is simpler and more scalable than that for viral vectors, making them easier to produce and more cost-effective. They have a better safety profile and undergo a simpler regulatory pathway. This can facilitate the approval process and expedite the production timeline. Another advantage of non-viral vectors is that they can be designed to specifically target T cells. For example, NPs engineered through specific receptors such as CD3 or CD28 increases the efficiency of gene delivery and reduces the potential for off-target effects (Lukjanov et al., 2021). In addition, they can be modified to improve their stability and bioavailability. Non-viral vectors also have the potential to be more flexible than viral vectors. They can be easily modified to carry different types of genes or to target different cell types, making them adaptable to a wide range of applications. This flexibility also means that non-viral vectors can be optimized for specific therapeutic goals, such as maximizing CAR expression levels (Ramamoorth & Narvekar, 2015).
Safety
NPs have several advantages that make them attractive for gene delivery to T cells, including their ability to go undetected by the immune system, biodegradability, sustainability to produce in mass quantities, and clinical advancements.
One of the main advantages of CAR gene carrying NPs is that they can go undetected by the immune system. This is because NPs can be designed to mimic natural particles, such as lipids or proteins, which the body is already familiar with. Additionally, NPs can be engineered to have a size and shape that allows them to bypass the immune system’s defenses and reach their intended target cells. This means that the NPs can deliver their cargo, the CAR genes, to the T cells without triggering an immune response, reducing the risk of adverse effects (Bhirde et al., 2011). Another advantage is that they are biodegradable. This means that once the NPs have delivered their cargo, they will naturally degrade in the body, leaving no toxic or harmful residues. This is in contrast to conventional CAR T cells, which can potentially persist in the body and cause adverse effects, such as cytokine release syndrome or neurotoxicity. By using biodegradable NPs, the risk of these adverse effects is significantly reduced (Est-Witte et al., 2021). Moreover, NPs are sustainable to produce in mass quantities. Unlike conventional CAR T cells, which require the extraction of T cells from the patient, genetic engineering, and expansion in culture, NPs can be produced in large quantities using standard manufacturing processes. This makes the production of CAR gene carrying NPs more efficient, cost-effective, and scalable, allowing for wider accessibility to patients (Abbasi et al., 2022).
CAR gene carrying NPs for T cell gene delivery have seen clinical advancements. In recent years, several clinical trials have been conducted to test the safety and efficacy of NPs for gene delivery to T cells. These trials have shown promising results, with evidence of improved outcomes and fewer adverse effects compared to conventional CAR T cell therapy. Moreover, new advances in NP design and manufacturing are further increasing the potential of CAR gene carrying NPs for T cell gene delivery as a safe and effective approach to cancer therapy (Xin et al, 2022).
Discussions
One major challenge is the limited transfection efficiency of the NPs, which can result in low expression levels of the CAR protein on the T cell surface. This can lead to reduced cytotoxicity against cancer cells and limit the therapeutic efficacy of the treatment (Dimitri et al., 2022). To overcome this challenge, CRISPR-Cas9 gene editing can be used to enhance the expression of the CAR gene in T cells. By using CRISPR technology to target specific genomic loci that regulate CAR expression, it can increase the transcriptional activity of the CAR gene and improve the expression levels of the CAR protein on the T cell surface. This approach has been shown to enhance the anti-tumor efficacy of CAR T cells in preclinical models (Moretti et al., 2022). Another challenge with CAR NPs is the potential for unintended gene editing. The use of CRISPR gene editing to address this challenge involves developing specific guide RNAs that target only the intended genomic loci. The use of a split-Cas9 system can help reduce the risk of off-target effects by requiring two separate components to come together to induce gene editing (Nie et al., 2022). In the case of adverse immune reactions, CRISPR can target specific genomic loci associated with the immune system to silence or edit genes that may trigger an immune response against the CAR NPs. This can improve the safety and efficacy of the treatment by reducing the likelihood of unintended reactions (Dimitri et al., 2022).
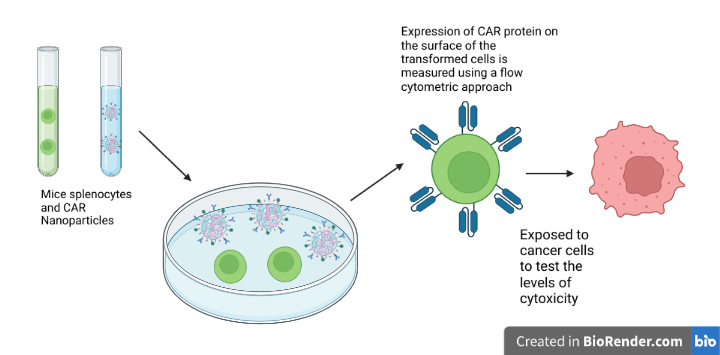
| Figure 6. Process of testing the efficiency and measuring effectiveness of CAR nanoparticles in mice splenocytes. |
|---|
Next Steps
An in vitro approach can be used to test this design. Isolated mouse splenocytes can be activated using a mitogen or antigen. Then, the activated splenocytes will be cultured in the presence of NPs containing a plasmid carrying the CAR genes (Fig. 6)(Smith et al., 2017).
After culturing the splenocytes with the CAR NPs, the expression of the CAR protein on the surface of the cells using a flow cytometric approach will be measured to determine whether the CAR genes have successfully been delivered to the splenocytes and whether they have been expressed. It can also measure the proliferation and differentiation of the splenocytes into effector T cells, which is a key characteristic of T cells activated by CAR T celltherapy (Smith et al., 2017). Exposing the splenocytes to cancer cells expressing the target antigen of the CAR will test their specificity. Measuring the cytotoxicity of the splenocytes against the cancer cells will determine whether the CAR NPs have successfully induced an immune response against the cancer cells (Lukjanov et al., 2021).
Acknowledgements
I would like to thank Ms. Lindsey L’Ecuyer for her constant commitment to her student’s passion in synthetic biology, and for always being willing to help out anytime no matter the circumstances. She was the one who had introduced me to the world of synthetic biology and has initiated an unwavering enthusiasm for me to further pursue the career in detail.
This project was accomplished through participation in the BioBuilderClub, an after-school program organized by BioBuilder Educational Foundation. BioBuilderClub engages high school teams around the world to combine engineering approaches and scientific know-how to design/build/test their own project ideas using synthetic biology.
References
Abbasi, S., Totmaj, M. A., Abbasi, M., Hajazimian, S., Goleij, P., Behroozi, J., Shademan, B., Isazadeh, A., & Baradaran, B. (2022). Chimeric antigen receptor T (CAR‐T) cells: Novel cell therapy for hematological malignancies. Cancer Medicine. 12(7), 7844-7858. https://doi.org/10.1002/cam4.5551
Albinger, N., Hartmann, J., & Ullrich, E. (2021). Current status and perspective of CAR-T and CAR-NK cell therapy trials in Germany. Gene Therapy, 28(9), 513-527. https://doi.org/10.1038/s41434-021-00246-w
Atsavapranee, E. S., Billingsley, M. M., & Mitchell, M. J. (2021). Delivery technologies for T cell gene editing: Applications in cancer immunotherapy. EBioMedicine, 67. 103354. https://doi.org/10.1016/j.ebiom.2021.103354
Balakrishnan, P. B., & Sweeney, E. E. (2021). Nanoparticles for enhanced adoptive T cell therapies and future perspectives for CNS tumors. Frontiers in Immunology, 12, 600659. https://doi.org/10.3389/fimmu.2021.600659
Bhirde, A., Xie, J., Swierczewska, M., & Chen, X. (2011). Nanoparticles for cell labeling. Nanoscale, 3(1), 142-153. https://doi.org/10.1039/C0NR00493F
Cleveland Clinic. (2023, January 17). T-Cells: Types and function. https://my.clevelandclinic.org/health/body/24630-t-cells
Dimitri, A., Herbst, F., & Fraietta, J. A. (2022). Engineering the next-generation of CAR T-cells with CRISPR-Cas9 gene editing. Molecular Cancer, 21(1), 78. https://doi.org/10.1186/s12943-022-01559-z
Est-Witte, S. E., Livingston, N. K., Omotoso, M. O., Green, J. J., & Schneck, J. P. (2021, August). Nanoparticles for generating antigen-specific t cells for immunotherapy. Seminars in Immunology, 56, 101541. https://doi.org/10.1016/j.smim.2021.101541
Hou, A. J., Chen, L. C., & Chen, Y. Y. (2021). Navigating CAR-T cells through the solid-tumour microenvironment. Nature Reviews Drug Discovery, 20(7), 531-550. https://doi.org/10.1038/s41573-021-00189-2
Lukjanov, V., Koutná, I., & Šimara, P. (2021). CAR T-cell production using nonviral approaches. Journal of Immunology Research, 2021. https://doi.org/10.1155/2021/6644685
Moretti, A., Ponzo, M., Nicolette, C. A., Tcherepanova, I. Y., Biondi, A., & Magnani, C. F. (2022). The past, present, and future of non-viral CAR T cells. Frontiers in Immunology, 13, 867013. https://doi.org/10.3389%2Ffimmu.2022.867013
National Cancer Institute. (2022, March 10). CAR T cells: Engineering immune cells to treat cancer. https://www.cancer.gov/about-cancer/treatment/research/car-t-cells
Nie, D., Guo, T., Yue, M., Li, W., Zong, X., Zhu, Y., Huang, J., & Lin, M. (2022). Research progress on nanoparticles-based CRISPR/Cas9 system for targeted therapy of tumors. Biomolecules, 12(9), 1239. https://doi.org/10.3390%2Fbiom12091239
Ramamoorth, M., & Narvekar, A. (2015). Non viral vectors in gene therapy-An overview. Journal of Clinical and Diagnostic Research: JCDR, 9(1), GE01-GE06. https://doi.org/10.7860%2FJCDR%2F2015%2F10443.5394
Shin, S., Lee, P., Han, J., Kim, S. N., Lim, J., Park, D. H., Paik, T., Min, J., Park, C. G., & Park, W. (2023). Nanoparticle-based chimeric antigen receptor therapy for cancer immunotherapy. Tissue Engineering and Regenerative Medicine, 20, 371-287. https://doi.org/10.1007/s13770-022-00515-8
Smith, T. T., Stephan, S. B., Moffett, H. F., McKnight, L. E., Ji, W., Reiman, D., Bonagofski, E., Wohlfahrt, M. E., Pillai, S. P. S., & Stephan, M. T. (2017). In situ programming of leukaemia-specific T cells using synthetic DNA nanocarriers. Nature Nanotechnology, 12(8), 813-820. https://doi.org/10.1038/nnano.2017.57
Xin, T., Cheng, L., Zhou, C., Zhao, Y., Hu, Z., & Wu, X. (2022). In-vivo induced CAR-T cell for the potential breakthrough to overcome the barriers of current CAR-T cell therapy. Frontiers in Oncology, 12, 809754. https://doi.org/10.3389/fonc.2022.809754
Zhang, Z. Z., Wang, T., Wang, X. F., Zhang, Y. Q., Song, S. X., & Ma, C. Q. (2022). Improving the ability of CAR-T cells to hit solid tumors: Challenges and strategies. Pharmacological Research, 175, 106036. https://doi.org/10.1016/j.phrs.2021.106036