Adrian Alfirevic, Abbi Bernhardt, Gavin Gall, Ben Grant, and Kaden Haslinger, Western Reserve Academy, Hudson, Ohio, United States
Reviewed on 3 May 2025; Accepted on 9 June 2025; Published on 27 October 2025
With help from the 2025 BioTreks Production Team.
Eighteen million people worldwide suffer from rheumatoid arthritis (RA), a chronic autoimmune disease that causing swelling, inflammation, and damage to joint linings. In some rare cases, it can spread to other parts of the body. As of now, RA cannot be cured, but disease-modifying antirheumatic drugs (DMARDs) or nonsteroidal anti-inflammatory drugs (NSAIDs) are used to limit symptoms. However, DMARDs increase the risk of infection by suppressing the immune system, whereas NSAIDs should be used only in the short term. When inflammation occurs, the body responds by releasing high levels of nuclear factor-kappa B (NF-kB), a protein complex that promotes the expression of proinflammatory cytokines and chemokines. Our project aims to reduce the body’s inflammatory response to RA by developing a response mechanism utilizing NF-kB. This design engineers Lactobacillus to produce curcumin, the anti-inflammatory molecule derived from the plant Curcuma longa, to significantly reduce the inflammatory response. Our design becomes a self-regulating machine by pairing curcumin production with the NF-kB-inducible promoter JTi2. Our goal is to create an automatic regulator and responder to abnormal levels of inflammation in the body, serving as a long-term treatment for those suffering from RA and possibly other autoimmune disorders.
Keywords: Curcumin, rheumatoid arthritis, Lactobacillus, NF-kB, anti-inflammatory
Authors are listed in alphabetical order. Sitaram Meena and Beth Pethel mentored the group. Please direct all correspondence to pethelb@wra.net.
Background
Overview
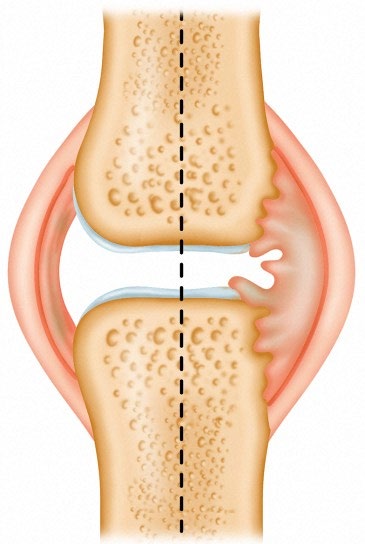
Rheumatoid arthritis (RA) is a chronic autoimmune disease that affects the joints and other parts of the body. When a person experiences RA, the immune system mistakenly attacks the synovium, which is the thin tissue lining inside the joints, causing swelling, pain, and cartilage damage. The damaged cartilage, a strong connective tissue, causes friction between the bones, which results in mobility issues and pain while moving that joint (Figure 1). RA mainly affects joints such as the fingers, wrists, knees, and ankles; however, RA can also affect vital organs like the heart, lungs, skin, eyes, and blood vessels (Overview on Rheumatoid, n.d.). Research has demonstrated that genetics, hormonal changes, or environmental factors could initiate the disease; however, no singular cause has been identified (Overview on Rheumatoid, n.d).
| Figure 1. Rheumatoid Arthritis affecting the joint finger: The left side displays a healthy finger, while the right side highlights the inflammation of the synovium. The swelling can lead to long-term pain and stiffness if left untreated. |
|
certain risk factors are present in developing RA, such as family history, smoking, obesity, and gender (Rheumatoid Arthritis, n.d.). A key molecule responsible for RA is interleukin 1 (IL-1), an inflammatory cytokine that mediates bone degradation and cartilage damage (Schiff, 2000) through the NF-kB signaling pathway. NF-kB binds to the DNA and promotes the expression of genes involved in inflammation, leading to the upregulation of an inflammatory response.
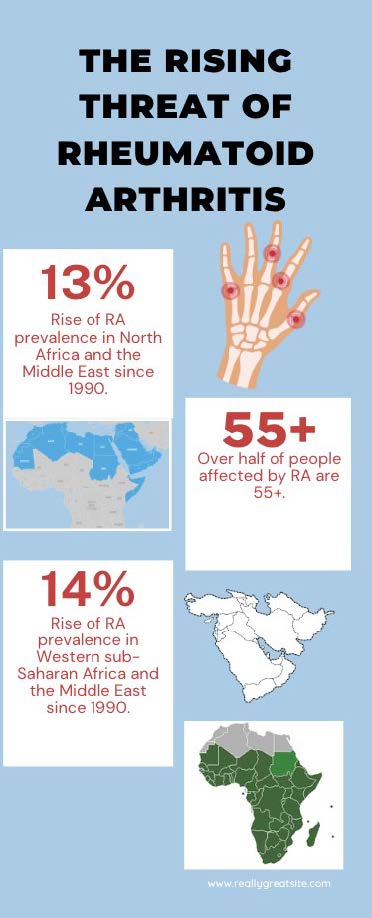
| Figure 2. The threat of Rheumatoid Arthritis is increasing throughout the world with nearly a 13% increase in cases since 1990. Over half of the people suffering from the disease are 55 years or older. |
|
Effect
Current treatments for RA aren’t as effective in dealing with the problem, and most long-term solutions have lasting side effects. Approximately 18 million people worldwide, including 1.5 million in the United States alone, currently have RA (World Health Organization, n.d). Early symptoms of RA are typically not specific to RA, such as fever, joint stiffness, and fatigue. For this reason, RA is typically not screened for early on unless symptoms are consistent for a few months. There is no one test to confirm if someone has RA. Still, researchers use blood and imaging tests to look for antibodies associated with RA, and MRIs and ultrasound tests to monitor damage done to joints (Mayo Clinic, n.d). If left untreated, RA can become substantially more severe. Symptoms in the later stages of RA include increased joint pain, decreased range of motion, and bone fractures (Carey & Lindenberg, 2024). The prevalence of RA (Figure 2) has increased in recent decades, with increases of 13% in North Africa and the Middle East and 14% in Western sub-Saharan Africa since 1990. Over half (55%) of those affected are 55 or older (Pfizer, 2023). RA also incurs significant expenses for treatment. In the United States patients pay $3,723 per year for a normal RA-specific treatment regimen and $20,262 for the more advanced bDMARD treatment (Hresko, 2018). The increasing prevalence, diagnostic challenges, disease severity, and high treatment costs stress the importance of creating more effective, earlier, and cheaper therapies for RA.
Treatment
RA cannot be cured, but some treatments help reduce symptoms and slow disease progression; early intervention can prevent further joint damage. The most commonly used treatments are disease-modifying antirheumatic drugs, or DMARDs. DMARDs reduce the production of inflammatory-causing chemicals in an immune response. and are typically made in a lab. Biologics used to treat RA target specific parts of the immune system to reduce inflammation and slow disease progression. These include TNF inhibitors, IL-6 inhibitors, B-cell depleting agents, T-cell co-stimulation blockers, and JAK inhibitors, each working through different immune pathways.(Rheumatoid Arthritis, n.d.). Biologics’ strength leads to a higher risk of side effects in the immune system (Rheumatoid Arthritis, n.d.). Biologics are given to a patient through an intravenous or IV infusion. DMARDS target the origin of inflammation and joint damage, preventing long-term damage and providing long-term relief (Disease-Modifying Antirheumatic, n.d.). Nonsteroidal anti-inflammatory drugs or NSAIDs can help slow its progression, but the long-term use of NSAIDs is limited due to gastrointestinal and cardiovascular side effects. NSAIDs block an enzyme called cyclooxygenase, which is important in producing prostaglandins (NSAIDs (Nonsteroidal, n.d.).. Prostaglandins are hormone-like compounds that play an important role in the body’s inflammation and regulation of other processes. NSAIDs remain an important option for short-term symptoms while waiting for DMARDs to take full effect in the body(NSAIDs (Nonsteroidal, n.d.).
|
Solution
Our proposed solution uses the anti-inflammatory properties of curcumin. We aim to pair it with a gut microbe and a promoter to enable the body to produce curcumin naturally during high levels of inflammation. Curcumin, which is naturally found in the turmeric plant, inhibits proinflammatory processes by suppressing the transcription of the cytokine genes. These cytokines are protein molecules that play a crucial role in regulating the immune system and influencing processes such as inflammation.
Our solution uses the anti-inflammatory properties of curcumin to autonomously activate within the body when high levels of NF-kB are present. The body would then regulate the curcumin production by using an engineered promoter (Part: BBa_K3661006). This part derives from the promoter JTi2 and would act as the on/off switch for the release of curcumin (Lu, 2020). Since JTi2 is inducible by NF-kB binding sites, the expression of the curcumin production genes will be activated in response to inflammation in the body. This anti-inflammatory response allows the engineered chassis to tightly regulate curcumin production based on the body’s inflammatory signals, particularly NF-KB levels.
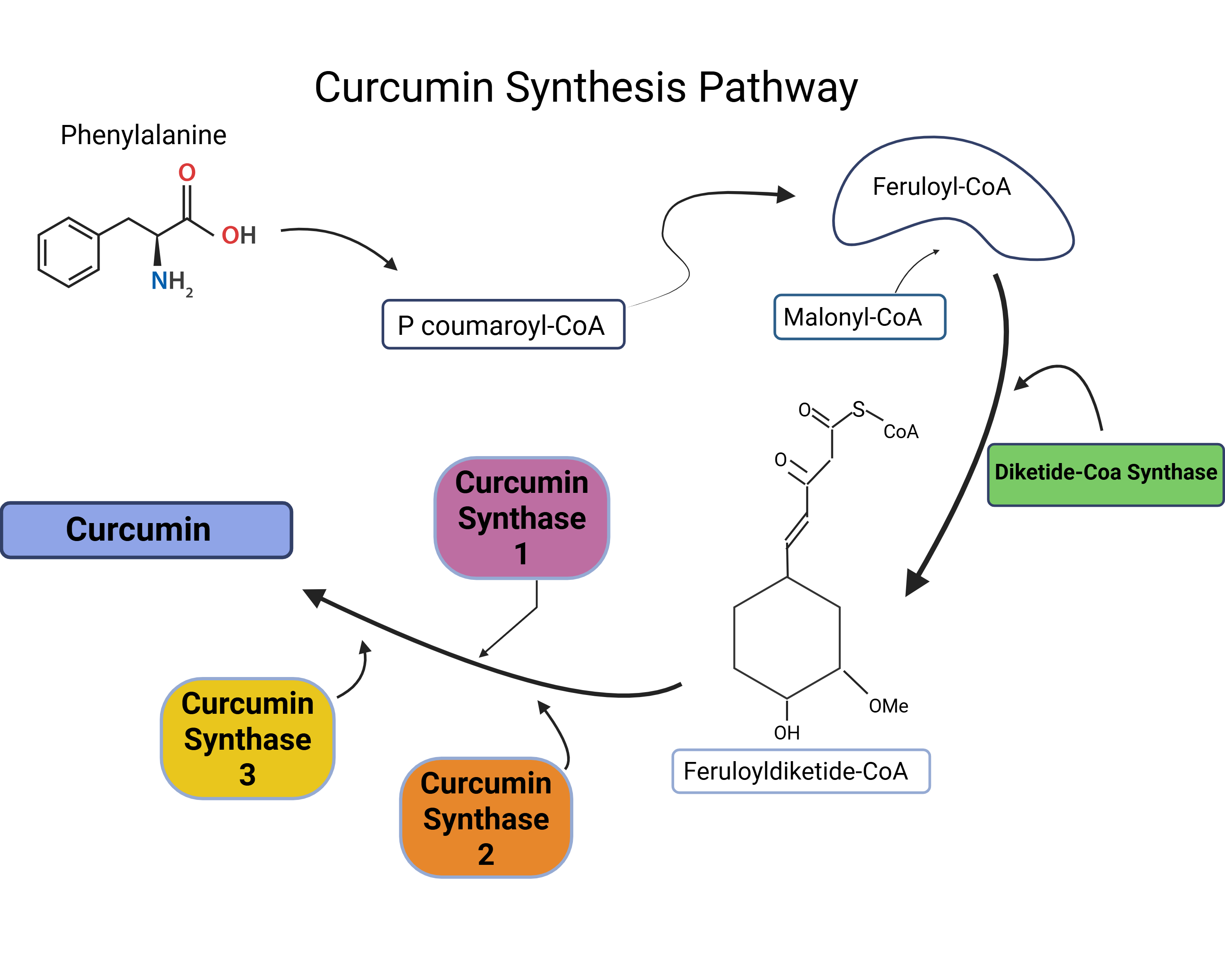
| Figure 3. The biosynthesis pathway leading to the production of curcumin involves the coordination of the CURS1, CURS2, CURS3, and DCS enzymes. These enzymes work to catalyze the essential steps to synthesis curcumin. |
|
Lastly, we will integrate the genes for curcumin synthase (CURS) 1, 2, 3, and diketide-CoA synthase (DCS) into our device to produce curcumin. (Figure 4.) The curcumin synthesis pathway will be incorporated into our plasmid pGK12.
Our plasmid is specifically designed for Lactobacillus (LGC), and we will use LGC because it naturally resides in the gut and is safe for human application. Additionally, our device will include the promoter JTi2, which is induced by the transcription factor NF-kB. This process creates an automated, responsive system where curcumin synthesis occurs at periods during high NF-kB levels, ultimately reducing the severityof rheumatoid arthritis. Because our system exists within the body, patients will not have to take recurring doses which will make it a cheaper treatment option. (Figure 4).
| Figure 4. The binding of the NF-kB complex activates the JTi2 promoter, triggering the expression of key enzymes CURS1, CURS2, CURS3, and DCS. These encode the genes necessary for the production and release of curcumin from Lactobacillus. |
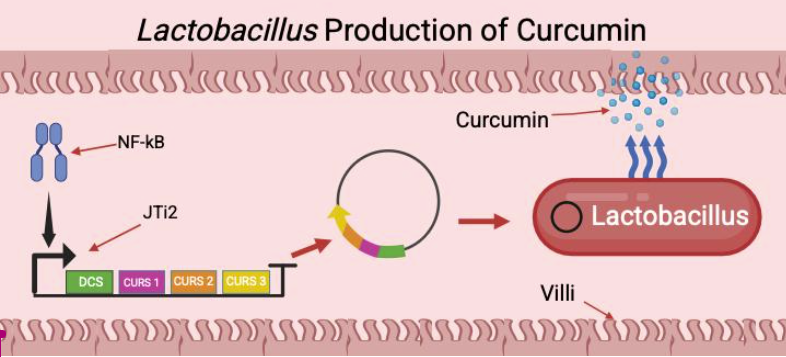
|
Systems Level
To create an innovative solution for delivering curcumin within the body, we chose to utilize Lactobacillus as our microbial organism. Lactobacillus is a gut bacterium with probiotic properties and the ability to increase curcumin bioavailability, a molecule with anti-inflammatory properties. By engineering Lactobacillus to secrete curcumin in the gut, we aim to overcome the inherent poor absorption of curcumin in the human body.
To achieve this, we will introduce the plasmid pWV01 containing the curcumin synthase genes (CURS 1-3) into Lactobacillus. We will test our engineered bacteria to make sure 1) they work and 2) they do not harm the human subject. This process will enable us to control the rate of engineered curcumin release while maintaining compatibility with the human body. Once Lactobacillus is inside the gut, it interacts with the NF-κB pathway and regulates inflammation. NF-κB, a transcription factor that promotes the production of proinflammatory cytokines, will activate our system when present. By delivering curcumin directly to the gut, Lactobacillus inhibits NF-κB activation and slows the production of inflammation. This downregulation of cytokines ultimately reduces inflammation and improves the progression of inflammatory diseases, such as rheumatoid arthritis.
Device Level
This design aims to engineer a working plasmid compatible with Lactobacillus which can be stably maintained within the organism. We plan to achieve this by integrating the erythromycin resistance (emr) gene from the plasmid pE194 Cop-6 into the plasmid pWV01. EMR was selected due to its high compatibility with Bacillus species and the fact that Lactobacillus is not resistant to erythromycin. The combined structure creates the plasmid pGK12. pWV01 serves as the backbone for our project because of its common compatibility with Bacilli species and its stable nature. Our improved plasmid will be tested in Lactobacillus and observed carefully in a laboratory setting to confirm the necessary genetic
modifications.
| Figure 5. pWV01 Plasmid. This is a rendering of our plasmid we plan to use. |
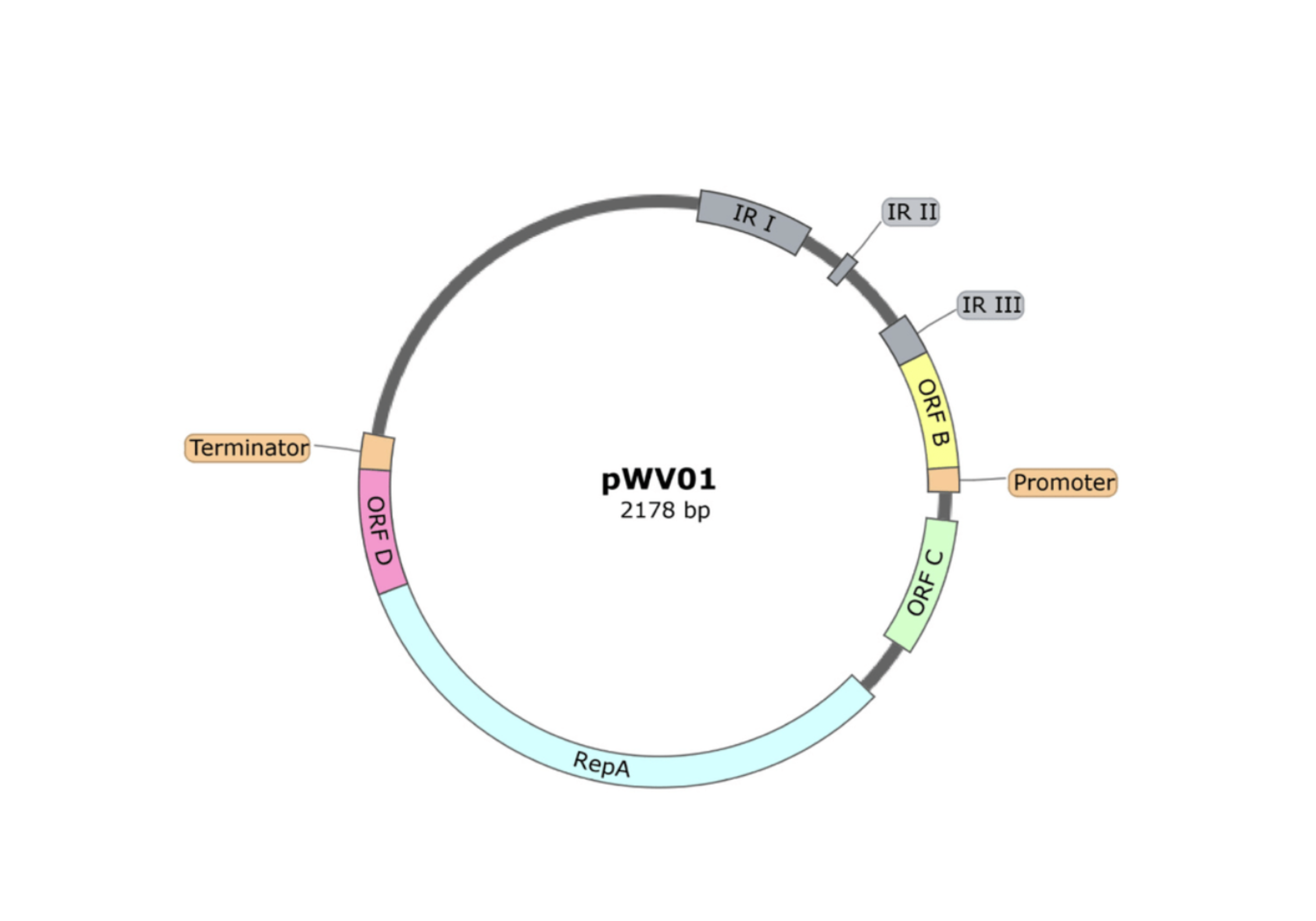
|
Promoter: JTi2
JTi2 is an NF-kB inducible promoter. In our system, it activates our device when NF-kB is present during the inflammatory process. It will activate the genes to produce curcumin.
Plasmid: pGK12 (pWV01 constructed with Emr taken from pE194 cop-6 variant)
We will use a plasmid developed by combining pWV01 (Streptococcus cremoris) with erythromycin resistance (EMR) from the pE194 cop-6 variant. This creates the pGK12 plasmid that is used to disrupt our genes by inserting new DNA fragments (Figure 2).
Enzymes: Curcumin synthase (CURS) 1,2,3 and diketide Co-A synthase (DCS).
These four enzymes work in combination to produce curcumin, the end product of our device, reducing inflammation. CURS accelerate the in vitro formation of curcuminoids to produce curcumin, and DCS is a critical enzyme that supports the production (Nguyen, 2018). They will be inserted into our plasmid to produce the necessary components for curcumin production. They are critical to the curcumin synthesis pathway.
Safety
Our starting organism , Lactobacillus acidophilus, is otypically found in the small intestine, where it plays a crucial role in the digestion of food. It produces hydrogen peroxide and lactic acid, substances that create an acidic environment that is unfavorable for harmful bacteria One of the most researched strains of L. acidophilus is the NCFM strain, which has been extensively tested in vitro and through human trials, with 45 clinical studies conducted. These studies have focused on various health aspects, including gastrointestinal health, immune function, antibiotic-associated gut disturbances, and irritable bowel syndrome. Since the 1970s, the NCFM strain has been used in the production of milk, yogurt, and toddler formula. Additionally, the NCFM strain is known for its ability to survive the gastrointestinal tract, making it a robust and viable candidate for curcumin production within the body. Based on research and applications in the food industry, we are confident that the NCFM strain of L. acidophilus will serve as a safe and viable chassis for curcumin production within the body.
Although our goal is to produce a constant supply of curcumin, it is vital to regulate this production as it can become harmful when excessive. If the body automatically produces curcumin in great amounts, it could interfere with the body’s natural immune responses, which are essential for proper healing. Additionally, curcumin may be harmful to helpful microorganisms within the body, potentially harming a person’s microbiome and interfering with bodily functions such as digestion. Curcumin also suppresses NF-κB, a key regulator in the body’s detoxification system. If NF-kB is over-suppressed due to high curcumin doses, the liver may be unable to metabolize curcumin, leading to possible digestive issues that might damage both the liver and gut cells. These issues would stem from inadequate regulation of curcumin production, making it necessary to conduct various tests to ensure proper control of the device.
Discussion
To turn our design into a consumer product, various tests would need to be performed to ensure the safety and feasibility of our design. We will start with lab-based quality control, meaning running PCR and sequencing the genes expressing the curcumin synthesis enzymes, quantifying our curcumin production and using qPCR to verify expression levels under simulated conditions. Another step would be to simulate conditions similar to those in the gut and grow the engineered Lactobacillus to determine if our design could survive and reproduce. If so, we will use high-performance liquid chromatography (HPLC) as a quantitative method to measure the curcumin levels produced. To further enhance the functionality of our design, we aim to utilize a model of SHIME (Simulator of Human Intestinal Microbial Ecosystem) to replicate gut conditions and introduce the engineered Lactobacillus into the simulated environment. HPLC will be used to detect the curcumin levels produced by the design. Finally, animal and human testing would begin with fecal sampling from animals and testing for curcumin levels, metabolites, and inflammation levels. The primary method for detecting positive results in humans is through blood testing, which checks the efficiency of gut absorption by measuring the levels of curcumin in plasma.
One major challenge in our engineered curcumin approach is addressing its poor bioavailability. Traditionally, much of curcumin becomes metabolized before it reaches the bloodstream, primarily due to its poor water solubility and rapid breakdown once absorbed. As a result, only a small fraction is bioavailable Our solution to this problem lies in the blueprint of the engineered curcumin itself, which involves producing curcumin directly in the gut. We plan to test this bioavailability through pharmacokinetic analysis of blood and urine samples collected from patients with the engineered curcumin microbe.
Next Steps
In the future, we will focus on optimizing and adjusting the curcumin yield through tuning the promoter and optimizing the Lactobacillus chassis. We would compare the rate at which curcumin is produced through our modified Lactobacillus versus oral curcumin supplements. Regarding steps to ensure safety, if our design proves to be functional in the human gut, we will perform long-term gut microbe composition tests to detect any long-term effects on the host. If curcumin synthesis proves to be useful in treating RA, we could consider adding demethoxycurcumin (DMC), a derivative of curcumin that exhibits greater chemical stability and goes beyond RA with its potential antitumor properties. We would integrate DMC into our design to expand its market potential and begin designing a capsule for ingestion, followed by clinical testing and trials.
Author Contributions
The main idea of our project to combat RA using a self-regulating system within the body was made by G.G. All group members contributed to writing our abstract. We broke up our background into parts; A.A. wrote the Overview, B.G. wrote the Effect section, A.B. wrote the Treatment section, and G.G. and K.H wrote the Solution section.. G.G. wrote the Systems and Next Step sections and K.H., B.G., and K.H. wrote the Parts Level section. B.G., K.H. and A.B. collaborated to complete the Safety section, and A.A.and G.G. collaborated to write the Safety and Discussion sections. A.A. handled all references.
Acknowledgements
First, we’d like to acknowledge our teacher, Dr. Beth Pethel, who provided valuable insight, structure, and guidance throughout this process. Dr. Pethel taught us the foundational science of synthetic biology, giving us the necessary background to understand what we were researching and how it would come together.
We want to acknowledge our mentor, Dr. SitaRam Meena. After meeting with him over Zoom, we developed a better sense of the direction we wanted to go in for our project. Dr. Meena challenged us to think more critically about the strengths and limitations of our project, giving us a clearer vision of how our project should look.
References
Carey, E., & Lindenberg, S. (n.d.). What is the rheumatoid arthritis severity scale? (K. Weiss, Ed.). Healthline. https://www.healthline.com/health/rheumatoid-arthritis-severity-scale
Disease-modifying antirheumatic Drugs (DMARDs). (n.d.). Cleveland Clinic. https://my.clevelandclinic.org/health/treatments/disease-modifying-antirheumatic-drugs-dmards
Guo Q., Jin Y., Chen X., Ye X., Shen X., Lin M., Zeng C., Zhou T., Zhang J. (2024). NF-κB in biology and targeted therapy: new insights and translational implications. Signal Transduct Target Ther., 4(9):53. doi: 10.1038/s41392-024-01757-9.
Hresko, A., Lin, J., & Solomon, D. H. (2018). Medical Care Costs Associated with Rheumatoid Arthritis in the US: A Systematic Literature Review and Meta-analysis. Arthritis Care Res (Hoboken), 70(10):1431-1438. doi: 10.1002/acr.23512
Katz, J. N., Smith, S. R., Collins, J. E., Solomon, D. H., Jordan, J. M., Hunter, D. J., Suter, L. G., Yelin, E., Paitel, A. D., & Losina, E. (2016). Cost-effectiveness of nonsteroidal anti-inflammatory drugs and opioids in the treatment of knee osteoarthritis in older patients with multiple comorbidities. Osteoarthritis Cartilage, 24(3):409-18. doi: 10.1016/j.joca.2015.10.006
Kohls, K. (2024, February 3). Using Turmeric as an Anti-Inflammatory. UnityPointHealth. https://www.unitypoint.org/news-and-articles/using-turmeric-as-anti-inflammatory
Lu, W. (n.d.). Registry for Standard Biological Parts. IGEM. https://parts.igem.org/Part:BBa_K3661006
Mandel, D. R., Eichas, K., & Holmes, J. (2010). Bacillus coagulans: a viable adjunct therapy for relieving symptoms of rheumatoid arthritis according to a randomized, controlled trial. BMC Complement Altern Med,
.12(10),1.doi: 10.1186/1472-6882-10-1
Nguyen, L. (2008). The biosynthetic pathway of curcuminoid in turmeric (Curcuma longa) as revealed by 13C-labeled precursors. Biosci Biotechnol Biochem, 72(7):1789-98. doi: 10.1271/bbb.80075
NSAIDs (Nonsteroidal Anti-Inflammatory Drugs). (n.d.). Cleveland Clinic. https://my.clevelandclinic.org/health/treatments/11086-non-steroidal-anti-inflammatory-medicines-nsaids
Overview on rheumatoid arthritis. (n.d.). Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/rheumatoid-arthritis/symptoms-causes/syc-20353648
Rheumatoid arthritis. (n.d.). Retrieved November 8, 2024, from https://www.pfizer.com/disease-and-conditions/rheumatoid-arthritis
Rheumatoid arthritis. (n.d.). https://www.mayoclinic.org/diseases-conditions/rheumatoid-arthritis/diagnosis-treatment/drc-20353653
Rheumatoid arthritis. (2023, June 28). World Health Organization. Retrieved November 8, 2024, from https://www.who.int/news-room/fact-sheets/detail/rheumatoid-arthritis
Rheumatoid Arthritis in Finger Joint [Image]. (n.d.). https://www.flickr.com/photos/myarthritis/8882225136Schiff, M.H. (2000). Role of interleukin 1 and interleukin 1 receptor antagonist in the mediation of rheumatoid arthritis. Ann Rheum Dis., 59(Suppl 1),i103-8. doi: 10.1136/ard.59.suppl_1.i103.