Aarav Arora, Chelsea Alonzo-Francis, Ismail Farid Allauddin Khan Ghori, Riya Gupta, Anika Tapshalkar, and Aarya Thakkar – Denmark High School, Alpharetta, Georgia, United States of America
Reviewed on 3 May 2025; Accepted on 9 June 2025; Published on 27 October 2025
With help from the 2025 BioTreks Production Team.
Tuberculosis is one of the world’s leading bacterial infections caused by Mycobacterium tuberculosis (M. tuberculosis). It is contracted through the air and targets the lungs, and if left untreated, the disease may be fatal. With over 2.5 million cases just in Central Africa and over 400 thousand deaths each year, it is the second leading cause of death in the region. In this predominantly rural area, the primary identification method for this disease is a molecular diagnostic test called GeneXpert, which requires several hours to run, exacerbating the disease’s progression. The design explored in this paper–TB-EZ–modified a traditional lateral flow assay to create a rapid antigen test that utilized capillary action.
With this test, the goal was to detect the cell wall protein of M. tuberculosis, Ag85, as the antigen. This was achieved by designing a buffer that would lyse the M. tuberculosis bacteria so that the Ag85 antigen could be released for the antibody to bind to. The first antibody, EPR28401-54, would bind to gold nanoparticles and rest on a nitrocellulose membrane, which is porous and nonpolar to help facilitate capillary flow. Unsweetened milk powder was used as a surfactant for the nitrocellulose membrane to prevent protein complexes from binding to the membrane at undesired locations. As the antibody-gold complex traveled to the detection line, it would bind with another antibody, and the gold nanoparticles would be released. This then produces a color for visual identification. Through further research, interactions between the antibody, surfactants, blocking agents, and lysis buffer will be tested for more precise results. This test has the potential to affordably and efficiently reduce deaths caused by the pathogen through the rapid detection of M. tuberculosis to allow for further action to be taken immediately.
Keywords: Tuberculosis, rapid antigen testing, lateral flow assay, Ag85, Central Africa
Authors are listed in alphabetical order. Mary Cartenuto and Peter Horanyi mentored the group. Please direct all correspondence to mcartenuto@forsyth.k12.ga.us.




Background
In 2023, an estimated 10.8 million people fell ill with tuberculosis worldwide (Goletti et. al, 2025). In Central Africa, tuberculosis is the second leading cause of death, with a staggering 2.5 million cases and over 400 thousand deaths each year(Martial et. al, 2021; World Health Organization, 2024). The burden is especially severe in rural communities, and despite it being a preventable and curable disease, tuberculosis continues to ravage vulnerable populations where public health infrastructure is fragile and access to quality healthcare is limited. The continued devastation of tuberculosis in Central Africa is not due to a lack of medical knowledge or treatment options, but rather to systemic barriers that make access to diagnosis and care nearly impossible for millions (Hershfield, 2024). While antibiotics can cure tuberculosis, they are only effective when the disease is detected early and accurately (Davis et. al, 2014). This first step—diagnosis—is where the greatest collapse in care often occurs. In rural areas of Central Africa, healthcare infrastructure is extremely limited (Martial et. al, 2021). Many communities are located hours or even days from the nearest medical facility, and public transportation is unreliable or nonexistent (Ag85B, 2016; Oleribe et. al, 2019). Even where clinics do exist, they often lack electricity, refrigeration, and trained personnel, making sophisticated diagnostic tools pointless. Traditional tuberculosis diagnostics like sputum smear microscopy and culture require both time and laboratory resources, lasting up to eight weeks to produce results (Chandra et.al, 2015). This is a delay that gives the disease time to worsen and spread (Narita et. al, 1998).
| Figure 1. |
|
Modern alternatives, like GeneXpert machines, use nucleic acid amplification to detect M. tuberculosis DNA. While faster and more accurate, GeneXpert is expensive. These devices also require stable electricity and routine maintenance (Davis et. al, 2014; Saeed et. al, 2017)—luxuries that many clinics in high-burden areas cannot afford (Stevens et. al, 2017). The consequence is that diagnosis remains a luxury, not a guarantee, and tuberculosis continues to spread unchecked. Beyond infrastructure, the human element adds another layer of complexity. Many patients are never tested simply because they cannot afford to miss a day of work to travel, or because they fear the social stigma of being labeled as “sick.”
Recognizing these obstacles, we developed TB-EZ, a non-invasive, swab-based diagnostic tool designed specifically for use at the point of care. The device is intended to detect tuberculosis biomarkers—specifically the Antigen 85 complex (Ag85), a group of proteins that make up the cell wall of the Mycobacterium tuberculosis (M. tuberculosis)bacteria (Bentley‐Hibbert et. al, 1999; Favrot et. al, 2013; Karbalaei Zadeh Babaki et. al, 2017). It is designed to be a tool that is lightweight, inexpensive, and easy to use, while producing accurate results within mere minutes, reducing delays between testing and treatment initiation. By tailoring diagnostic capabilities to the realities of the high-burden, low-resource settings, the project addresses one of the most persistent gaps in global tuberculosis care. In areas where every delay in diagnosis can mean the difference between containment and transmission—or between survival and death—such a tool has the potential to transform outcomes at both the individual and community level.
Systems level
The diagnostic swab was designed to detect tuberculosis by targeting Ag85, a protein complex that is naturally found in the M. tuberculosis bacterium and released during infection (Bentley‐Hibbert et. al, 1999). Because this bacterium is commonly present in bodily fluids like saliva or mucus during active infection (Schmidt-Schultz and Schultz, 2015), the swab can collect a sample to test for Ag85 non-invasively. Once the sample is collected, a lysis buffer breaks down the bacterium’s cell wall, thus releasing the antigen complex. These antigens then interact with the engineered gold-labeled antibodies that are embedded in the test strip; if Ag85 is present, the antigen-antibody complex will cause a visible color change at the detection line, thus indicating a positive result and confirming the presence of M. tuberculosis. On the other hand, if there is no Ag85 detected in the sputum sample—either because the patient is uninfected or the antigen is not present in sufficient amounts—the antigen-antibody complex will not cause a color change at the detection line, resulting in a negative result.
Device level
This test uses multiple device components that work together to detect Ag85; these include the buffer, nitrocellulose membrane, and lateral flow assay (LFA).
The buffer used in the test is made up of Tris-HCl (1.10 mM), sodium chloride (2.150 mM), and Tween 80 (0.1%). Tris-HCl is a common biological buffer used in diagnostic tests (Biocompare, 2024). Its primary function is to prevent overshooting of the pH, providing a stable environment for protein interactions (Armstrong, 2008). This is very important because an extreme pH can denature Ag85, ultimately impairing its compatibility. The sodium chloride solution maintains an optimal ionic strength that encourages antibody-antigen interactions (Armstrong, 2008). It also prevents non-specific interactions with other components of the test. Tween 80 lyses the cell membrane of M. tuberculosis by acting as an emulsifier and stabilizer (Armstrong, 2008; Payeur, 2014). The low concentration in this buffer maintains the integrity of Ag85 by preventing protein denaturation, therefore keeping it detectable. Tween 80 increases the solubility of lipids in the tuberculosis membrane due to its amphipathic properties, which allow it to interact with both water and lipids. This results in the formation of micelles that allow the lipids to be dispersed instead of settling out (Payeur, 2014; Sigma Aldrich, 2025). Tween 80 also acts as a surfactant, which prevents the antibodies from binding to the wrong areas on the nitrocellulose membrane (Boehringer, 2025; Pokhrel et. al, 2023). All these components allow Ag85 to be extracted from the cell membrane of M. tuberculosis for detection by the rest of the test. Because of the components of the buffer, the solution of the extracted Ag85 and lysis buffer will flow down the nitrocellulose membrane without interference.
The nitrocellulose membrane is primarily composed of purified cellulose that has been esterified with nitric acid, forming a fibrous, porous polymer. The base cellulose makes the nitrocellulose more hydrophobic and chemically active (Nurazzi et. al, 2023). Nitrocellulose membranes retain the ability of cellulose to bind proteins (Spiess et. al, 1981) more efficiently as it is esterified with nitric acid—the source of the nitro groups which are used in nitration (Morris et. al, 2024; Nurazzi et. al, 2023). Nitration modifies the cellulose structure, turning it into nitrocellulose, which is better for binding proteins and supporting fluid flow in membranes like those used in Western blots and other diagnostic tests. In LFAs, the cellulose-derived structure allows for consistent capillary action (Balser et. al, 2004; Chemcess, 2024; Klein and Mentser, 1951). The smaller pores further encourage capillary flow, allowing the lysed sputum sample to flow down the test. Additionally, more surface area is available in smaller pores, allowing more antigens to bind to the antibody, which can increase signal intensity. Smaller pore size also provides sharper test lines, improving visual clarity for the user (Klein and Mentser, 1951).
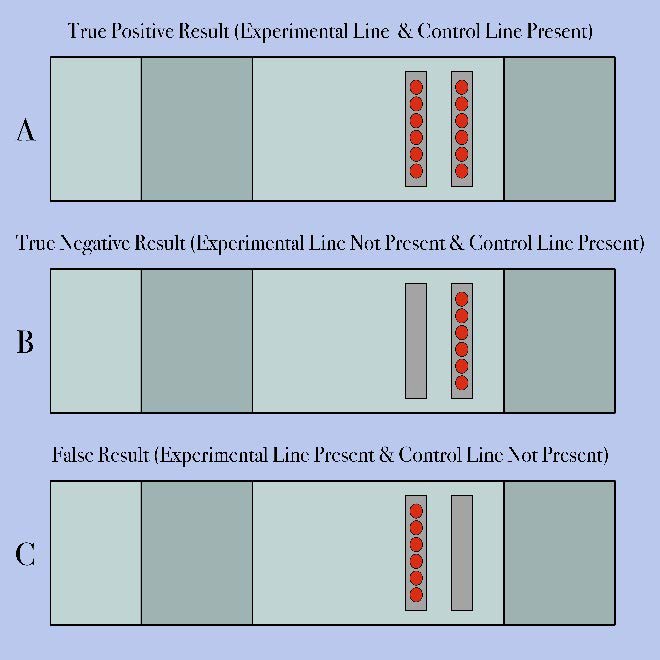
The TB-EZ test uses LFA to determine the presence of tuberculosis. LFAs allow antigens to combine with antibodies to indicate an outcome (Bahadir and Sezginturk, 2016; Leinco Technologies, n.d.). The solution of lysed bacteria and sputum moves through the pores of the nitrocellulose membrane through capillary action (Koczula and Gallotta; 2016). The Ag85 antigen in the sample will attach to the antibody, EPR28401-54, which is placed near the sputum sample. The antibody EPR28401-54 is coupled with the gold nanoparticle to create an antibody-gold nanoparticle complex. Then, the antigen-antibody complexes will move through the membrane and attach to the first bioengineered antibody. The first bioengineered antibody is specifically designed so that it binds exclusively to the antigen-antibody complex, which shows that tuberculosis is present. For non-antigen-antibody complexes, they will travel farther through the test and bind to the second bioengineered antibody. This antibody is specifically engineered to bind only to the antibody-gold nanoparticle complex. This is created as the control test to indicate if the test has worked successfully. The indication of the presence of tuberculosis through the detection of the antibody-antigen complex is shown through the surface plasmon resonance (SPR). The gold nanoparticles scatter light effectively (Dykman and Khlebtsov, 2011), producing a visible color; this is due to the electrons on their metal surface becoming excited at certain wavelengths of light (Hammami et. al, 2021, nanoComposix, 2022, Yeh et. al, 2012). The resonance of the first line will indicate the presence of the antigen, thus signifying infection. The resonance of the second line will indicate the functionality of the test.
| Figure 2. |
|
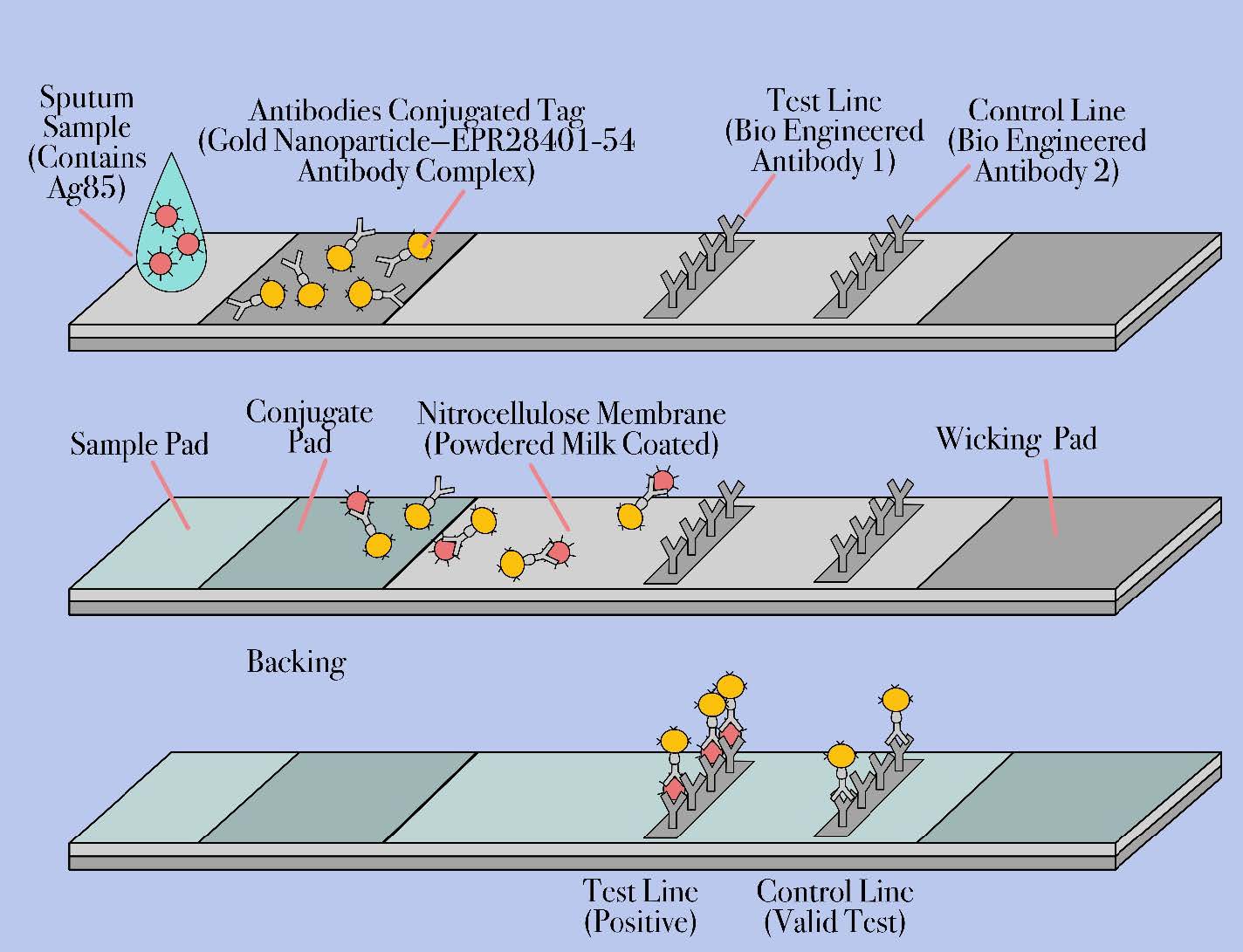
This diagram shows the mechanism by which the test works. Section A of the diagram depicts a TB-infected (therefore Ag85 containing) sputum sample initially contacting the sample pad. Section B of the diagram depicts the gold nanoparticle-EPR28401-54- antibody complexes binding to the Ag-85 antigens. Section C of the diagram depicts the antigen-antibody complex binding to the control and test line, indicating the individual has tuberculosis. The control line ensures functionality while the test line indicates the presence of Mycobacterium tuberculosis.
Parts level
The Ag85 protein complex is what is being tested, consisting of Ag85A, Ag85B, and Ag85C proteins (Bentley‐Hibbert et. al, 1999; Karbalaei Zadeh Babaki et. al, 2017, Kuo et. al, 2011). For this research paper, the main focus will be on the binding of Ag85B to EPR28401-54. Ag85B is a water-soluble protein and it has a hydrophilic surface, but its stability comes from its hydrophobic center. Ag85B is commonly found in mycobacterial walls because of its function as a mycolyl transferase. This means that Ag85B helps catalyze the transfer of mycolic acid to trehalose, forming trehalose dimycolate (Ag85B, 2016; Ernst, 2019) (TDM—a common glycolipid found in mycobacterial walls) (Faraz et. al, 2017; Payeur, 2014; Luo et. al, 2023; nanoComposix, 2022; Prendergast et. al, 2016; nanoComposix, 2016). Once a bacterium is lysed, this protein can be detected as it is a key structural component of a mycobacterium’s wall. Ag85B is highly immunogenic, meaning it elicits the strongest immune response out of the three proteins that make up the Ag85 complex. This is beneficial for diagnostic tests as it evokes stronger signals from detection antibodies (Ernst et. al, 2019; Armstrong, 2008; Faraz et. al, 2017). Additionally, Ag85B is secreted in higher concentrations by M. tuberculosis than Ag85A and Ag85C, so it will be in higher concentrations in the sputum sample, which increases the chances of the test being accurate (Murphy and Dempsey, 2020).
The antibody being used, EPR28401-54, is a specific monoclonal antibody developed for the detection of Ag85B from M. tuberculosis (Abcam, 2025). As part of the TB-EZ design, EPR28401-54 will bind to the Ag85B to help with rapid antigen testing—a form of diagnostic development. It is a safe antibody to use due to its non-reactivity with human proteins. It requires a relatively neutral pH environment (~7.4), with a mainly hydrophilic surface (Abcam, 2025; Biocompare, 2024), making it soluble in water-based buffers.
Gold nanoparticles (AuNPs) are bound to the Ag85B during the rapid antigen testing (RAT), which later accumulate on the unmodified EPR28401-54 antibody and the engineered version for tuberculosis detection of the antibody at the control line (Abcam, 2025; Sigma Aldrich, 2025; Waitkus et. al, 2022). The size of these particles is approximately 20 nm, which results in a pink-red color, due to surface plasmon resonance (SPR). AuNPs are not water soluble but have many methods of stabilization, such as surfactants, ligands, and polymers. However, they are naturally stable as they don’t oxidize or corrode easily in biological or chemical environments. AuNPs are commonly used in LFA (Bansal et. al, 2020) testing for diagnostic tests, and they are generally biocompatible if prepared correctly, posing no hazard to humans (nanoComposix, 2016; Sigma Aldrich, 2025).
By combining these three parts, a detection mechanism is created. The gold nanoparticle is bound to the Ag85B part of the antigen 85 protein complex (if present), where EPR28401-54 binds to Ag85B at the specific paratope. This creates a detection line on the nitrocellulose membrane, visible as a red line to users because of the SPR from the gold nanoparticles.
In this experiment, 3-5% nonfat milk powder will be used to prevent nonspecific binding to the nitrocellulose membrane (Sigma Aldrich, 2025). The milk protein contained in the powder sticks to the vacant surface area of the membrane, which prevents the non-specific binding of the antibodies. Milk powder is particularly good at “blocking” the membrane’s vacant surface area, as its wild mix of varied proteins provides particularly effective cover, which prevents non-specific binding (Hogan and O’Callaghan, 2010; Sigma Aldrich, 2025). Two specific proteins milk powder is composed of are caseins (insoluble) and whey proteins (soluble). Caseins make up about 80% of the total protein content (Madureira et. al, 2007). Casein effectively prevents nonspecific binding in biological assays by saturating available binding sites on surfaces like membranes or plastic, thus preventing the binding of primary and secondary antibodies to those sites. Casein also functions as a stabilizing protein, thus making it likely for the Ag85 and the EPR28401-54 to denature (Khatun et. al, 2022). Whey protein can impact nonspecific binding proteins by affecting their interactions and functions (Khatun et. al, 2022; Whey processing, 2007).
Safety
This system in this project is designed to prioritize user safety by addressing both the nature of tuberculosis and incorporating inactivation mechanisms during the testing process. Tuberculosis is transmitted exclusively through airborne particles and can cause fatal disease, which will mean that research and development for this test will require a BSL-3 lab (CDC, 2024). To further ensure the safety of the user, the test utilizes a Tris-HCl (1.10 mM), sodium chloride (2.150 mM), and Tween 80 (0.1%) lysis buffer, which should disrupt the bacterial cell wall and kill the pathogen(Kolia-Diafouka et. al, 2018), which can be better determined after further testing. As a result of this mechanism, by the time the sample reaches the detection stage of the LFA, the tuberculosis sample has already been rendered non-infectious (Cell Lysis Buffers – US., n.d.; Islam, 2017).
Although the risk of transmitting the tuberculosis sample is already minimal, this test’s disposal process includes redundancy to better align with safety practices. While tuberculosis does not spread once lysed, the test will include airtight bags to dispose of the swabs and nitrocellulose membrane. This ensures that the tuberculosis is completely isolated from the external environment to prevent unnecessary concern about the presence of biological waste. Furthermore, users will be recommended to return the sealed bag according to local biohazard waste regulations to act as an added redundancy. However, due to the pathogen being killed during the test, the bag can safely be discarded in a household trash bin without posing a biological hazard.
Discussions
Tuberculosis most commonly occurs in areas of low development and resources, limiting many people to one health check-up per year, if at all (Brinzac et. al, 2023; Oleribe et. al, 2023). This means that the time they have with a physician is limited, eliminating all lengthy lab testing to identify certain diseases. However, along with time, money is also a factor. Common testing methods for tuberculosis are both time-consuming and costly, such as nucleic acid amplification tests like GeneXpert, which hinge on invasive sputum sampling or availability of high-cost, electricity-powered equipment and skilled personnel (Davis et. al, 2014; Saeed et. al, 2017; Stevens, et. al, 2017). These are luxuries unavailable in much of rural dispensaries in Central Africa, where poor infrastructure and underfunded health systems limit diagnostic capabilities. The TB-EZ diagnostic swab meets an urgent need in tuberculosis care by offering a rapid, non-invasive, and accessible test to use with populations in low-resource areas. Its development is an answer to a popular realization that existing tools are poorly adapted to real-world conditions in under-resourced neighborhoods. TB-EZ eliminates reliance on such equipment by providing an instrument employing a basic swab that makes sampling much easier. In addition to this, the TB-EZ test is designed to last only minutes, making it possible to have an almost immediate result on which to make clinical decisions and quickly link patients to care. On a public health level, this reduced timeframe from sample collection to initiation of treatment can significantly decrease the duration of infectiousness of active cases, lessening transmission risk and helping to terminate infection in densely populated households and communities.
A few challenges that should be carefully monitored are the tendency of nitrocellulose to not work properly in humid environments and the chance of false negatives. Nitrocellulose membranes are hydrophilic (Boehringer, 2025; Pokhrel et .al, 2023), meaning that increased water will cause the membrane to swell. In humid environments, there is a high chance of this occurring; this membrane instability ruins the effectiveness of the membrane, providing distorted results. However, it is unlikely that this will occur because most clinics have procedures to either combat this or have rooms made that have their environmental conditions controlled. The other challenge is the chance of false negatives. A physician could suspect a patient of TB, but if they are in the early stages of the disease, there is little growth of tuberculosis in the sputum. Though the person has tuberculosis, a false negative result would be produced. The test will require specific concentrations of the tuberculosis bacterium, and if not met, the test will not be able to detect it. Physicians will have to use this test when patients have mild symptoms, at the very least. Future improvements include modifying nitrocellulose so that it adapts to temperate climates better, like that of South Africa, adding an amplifying factor in the test itself that helps increase its sensitivity, increase in the sensitivity of the binding mechanisms of the antibodies, complexes, and antigen to decrease the duration of the test evaluation and improve the efficiency of the test, and creation of a cleansing solution within the test that can be activated after use to eliminate all biohazardous objects in the test so that the test can be safely thrown away.
Next steps
Plans will focus on evaluating the interaction between the second engineered antibody and the travelling antigen-antibody complex. This step is critical to confirm that the binding mechanism functions correctly under test conditions. Ensuring that the secondary antibody accurately recognizes and allows the complex to bind to it is essential for producing a reliable colorimetric signal and maintaining the specificity of the diagnostic tool. Additionally, the system’s performance will be refined by analyzing the concentrations of key components, including proteins, surfactants, blocking agents, and the lysis buffer. These factors significantly influence the efficiency and clarity of the results, as improper levels can lead to weak signals or false readings. The flow dynamics of the sample through the nitrocellulose membrane will also be examined to ensure smooth and consistent capillary action across all test conditions. To enhance the accuracy of antigen detection, antibody and antigen concentrations will be calculated based on proportional data drawn from established COVID-19 diagnostic methodologies. This is because these procedures provide a useful foundation to determine effective concentration ranges, contributing to a more sensitive and dependable result in tuberculosis detection. Finally, experimental validation of the theoretical design will be conducted to make sure that all components function together cohesively. Particular emphasis will be placed on whether the timing of capillary flow and antigen-antibody binding occurs within an optimal window. This testing phase will be essential to confirm that the device operates not only in controlled conditions but also in real-world settings where reliability and speed are crucial.
Author contributions
Author IA contributed to the Device level and Author contributions sections, the development of an initial design of the test, future improvements, and helped with referencing. Author CAF was responsible for the Device level section, the production of the accompanying video material, in-depth analysis of the lysis buffer composition and LFA, and preliminary research into detection methods. Author AA contributed to the Safety section, developed the test diagrams, decided on tuberculosis and the target location, and helped with referencing. Author RG developed the Parts level section, focusing on the component-level analysis, researched membrane and lysis buffer options, surfactant research, colorimetrics, research compatibility between test components, test conversion from viral to bacterial, and preliminary LFA and RAT research. Anika T. authored the Background, Systems level, Next steps,and References sections, co-authored the Parts level and Discussions sections, and helped with referencing. Aarya T. contributed to the Device level, Next steps, and Parts level sections, researching milk powder and the preliminary membrane, and helped with referencing. All researchers helped contribute to the preliminary research, the design, the Abstract section, and editing.
Acknowledgements
We would like to sincerely thank Dr. Peter Horanyi, Ph.D., for the time and knowledge he invested in our project. His expertise was truly invaluable to our team’s understanding of synthetic biology and the research process in general. This team would also be incomplete without our compassionate and ingenious mentor, Mrs. Mary Cartenuto. Her unwavering support and guidance have challenged us to think critically, stay curious, and push the boundaries of our research in ways we never would have imagined.
References
Goletti, D., Meintjes, G., Andrade, B. B., Zumla, A., & Shan Lee, S. (2025). Insights from the 2024 WHO Global Tuberculosis Report – More Comprehensive Action, Innovation, and Investments required for achieving WHO End TB goals. International Journal of Infectious Diseases, 150, 107325. https://doi.org/10.1016/j.ijid.2024.107325
Martial, N. T., Mubarik, S., & Yu, C. (2021). Long-term trends of tuberculosis incidence and mortality in four central African countries. Scientific Reports, 11(1). https://doi.org/10.1038/s41598-021-95967-8
World Health Organization. (2024). Tuberculosis. Www.who.int. https://www.who.int/health-topics/tuberculosis
Hershfield, E. S. (1991). Tuberculosis – Still a Major Health Problem. Canadian Journal of Infectious Diseases, 2(4), 131–132. https://doi.org/10.1155/1991/297605
Davis, J. L., Kawamura, L. M., Chaisson, L. H., Grinsdale, J., Benhammou, J., Ho, C., Babst, A., Banouvong, H., Metcalfe, J. Z., Pandori, M., Hopewell, P. C., & Cattamanchi, A. (2014). Impact of GeneXpert MTB/RIF on Patients and Tuberculosis Programs in a Low-Burden Setting. A Hypothetical Trial. American Journal of Respiratory and Critical Care Medicine, 189(12), 1551–1559. https://doi.org/10.1164/rccm.201311-1974oc
Ag85B. (2016). Prospecbio. https://www.prospecbio.com/ag85b
Oleribe, O. E., Momoh, J., Uzochukwu, B. S., Mbofana, F., Adebiyi, A., Barbera, T., Williams, R., & Taylor Robinson, S. D. (2019). Identifying key challenges facing healthcare systems in Africa and potential solutions. International Journal of General Medicine, 12(1), 395–403. https://doi.org/10.2147/IJGM.S223882
Chandra, Tj., Selvaraj, R., & Sharma, Y. (2015). Same day sputum smear microscopy for the diagnosis of pulmonary tuberculosis: Ziehl-Neelsen versus fluorescent staining. Journal of Family Medicine and Primary Care, 4(4), 525. https://doi.org/10.4103/2249-4863.174273
Narita, M., Ashkin, D., Hollender, E. S., & Pitchenik, A. E. (1998). Paradoxical Worsening of Tuberculosis Following Antiretroviral Therapy in Patients with AIDS. American Journal of Respiratory and Critical Care Medicine, 158(1), 157–161. https://doi.org/10.1164/ajrccm.158.1.9712001
Saeed, M., Ahmad, M., Iram, S., Riaz, S., Akhtar, M., & Aslam, M. (2017). GeneXpert technology. A breakthrough for the diagnosis of tuberculous pericarditis and pleuritis in less than 2 hours. Saudi Medical Journal, 38(7), 699–705. https://doi.org/10.15537/smj.2017.7.17694
Stevens, W. S., Scott, L., Noble, L., Gous, N., & Dheda, K. (2017). Impact of the GeneXpert MTB/RIF Technology on Tuberculosis Control. Microbiology Spectrum, 5(1). https://doi.org/10.1128/microbiolspec.tbtb2-0040-2016
Bentley‐Hibbert, S., Quan, X., Newman, T., Huygen, K., & Godfrey, H. P. (1999). Pathophysiology of Antigen 85 in Patients with Active Tuberculosis: Antigen 85 Circulates as Complexes with Fibronectin and Immunoglobulin G. Infection and Immunity, 67(2), 581–588. https://doi.org/10.1128/iai.67.2.581-588.1999
Favrot, L., Grzegorzewicz, A. E., Lajiness, D. H., Marvin, R. K., Boucau, J., Isailovic, D., Jackson, M., & Ronning, D. R. (2013). Mechanism of inhibition of Mycobacterium tuberculosis antigen 85 by ebselen. Nature Communications, 4(1). https://doi.org/10.1038/ncomms3748
Karbalaei Zadeh Babaki, M., Soleimanpour, S., & Rezaee, S. A. (2017). Antigen 85 complex as a powerful Mycobacterium tuberculosis immunogene: Biology, immune-pathogenicity, applications in diagnosis, and vaccine design. Microbial Pathogenesis, 112, 20–29. https://doi.org/10.1016/j.micpath.2017.08.040
Schmidt-Schultz, T. H., & Schultz, M. (2015). AG 85, a major secretion protein of Mycobacterium tuberculosis, can be identified in ancient bone. Tuberculosis, 95, S87–S92. https://doi.org/10.1016/j.tube.2015.02.034
Tris-HCl Buffers | Biocompare. (2024). Biocompare.com. https://www.biocompare.com/pfu/111790/soids/1050505-2598556/Chemicals_and_Reagents/Buffers_Tris-HCl
Armstrong, B. (2008). Antigen–antibody reactions. ISBT Science Series, 3(2), 21–32. https://doi.org/10.1111/j.1751-2824.2008.00185.x
Payeur, J. B. (2014). Mycobacterium. Encyclopedia of Food Microbiology, 841–853. https://doi.org/10.1016/b978-0-12-384730-0.00229-9
Sigma Aldrich. (2025). NMR Chemical Shifts of Impurities. Merck, 1(1). https://www.sigmaaldrich.com/MX/en/technical-documents/technical-article/genomics/cloning-and-expression/blue-white-screening
Boehringer, H. (2025). Artemis Dx. Artemisdx.com. https://www.artemisdx.com/surfactants-lateral-flow-assays-part-1/
Pokhrel, D. R., Kumar Sah, M., Gautam, B., Kumar Basak, H., Bhattarai, A., & Chatterjee, A. (2023). A recent overview of surfactant–drug interactions and their importance. RSC Advances, 13(26), 17685–17704. https://doi.org/10.1039/d3ra02883f
Nurazzi, N. M., Shazleen, S. S., Norrrahim, M. N. F., Sabaruddin, F. A., Ilyas, R. A., Asyraf, M. R. M., Kamarudin, S. H., Naveen, J., & Sapuan, S. M. (2023). Molecular dynamics of nanocellulose-based nanocomposites: a review. Synthetic and Natural Nanofillers in Polymer Composites, 187–213. https://doi.org/10.1016/b978-0-443-19053-7.00008-1
Spiess, I., Blais, M., & Baumann, R. (1981, August 3). US4365059A – Nitration of cellulose – Google Patents. Google.com. https://patents.google.com/patent/US4365059A/en
Morris, E., Pulham, C. R., & Morrison, C. A. (2024). Towards understanding and directing the nitration of cellulose. Cellulose, 32(3), 1513–1526. https://doi.org/10.1007/s10570-024-06298-6
Balser, K., Hoppe, L., Eicher, T., Wandel, M., Astheimer, H., Steinmeier, H., & Allen, J. M. (2004). Cellulose Esters. Ullmann’s Encyclopedia of Industrial Chemistry. https://doi.org/10.1002/14356007.a05_419.pub2
Chemcess. (2024, January 16). Cellulose Nitrate: Properties, Production, And Uses. Industrial Production and Uses of Chemicals. https://chemcess.com/cellulose-nitrate-properties-production-and-uses/
Klein, R., & Mentser, M. (1951). The Mechanism of Cellulose Nitration1. Journal of the American Chemical Society, 73(12), 5888–5888. https://doi.org/10.1021/ja01156a529
Bahadır, E. B., & Sezgintürk, M. K. (2016). Lateral flow assays: Principles, designs and labels. TrAC Trends in Analytical Chemistry, 82, 286–306. https://doi.org/10.1016/j.trac.2016.06.006
Lateral Flow Assays: Principles, Designs and Reagents | Leinco. (n.d.). Leinco Technologies. https://www.leinco.com/lateral-flow-assay/
Koczula, K. M., & Gallotta, A. (2016). Lateral flow assays. Essays in Biochemistry, 60(1), 111–120. https://doi.org/10.1042/ebc20150012
Dykman, L. A., & Khlebtsov, N. G. (2011). Gold Nanoparticles in Biology and Medicine: Recent Advances and Prospects. Acta Naturae, 3(2), 34–55. https://doi.org/10.32607/20758251-2011-3-2-34-55
Hammami, I., Alabdallah, N. M., jomaa, A. A., & kamoun, M. (2021). Gold nanoparticles: Synthesis properties and applications. Journal of King Saud University – Science, 33(7), 101560. https://doi.org/10.1016/j.jksus.2021.101560
nanoComposix. (2022). Gold Nanoparticles: Optical Properties. NanoComposix. https://nanocomposix.com/pages/gold-nanoparticles-optical-properties
Yeh, Y.-C., Creran, B., & Rotello, V. M. (2012). Gold Nanoparticles: Preparation, Properties, and Applications in Bionanotechnology. Nanoscale, 4(6), 1871–1880. https://doi.org/10.1039/c1nr11188d
Kuo, C.-J., Bell, H., Hsieh, C.-L., Ptak, C. P., & Chang, Y.-F. (2011). Novel Mycobacteria Antigen 85 Complex Binding Motif on Fibronectin. Journal of Biological Chemistry, 287(3), 1892–1902. https://doi.org/10.1074/jbc.m111.298687
Ernst, J. D., Cornelius, A., & Bolz, M. (2019). Dynamics of Mycobacterium tuberculosis Ag85B Revealed by a Sensitive Enzyme-Linked Immunosorbent Assay. MBio, 10(2). https://doi.org/10.1128/mbio.00611-19
Faraz, A., Zubair, S., Gupta, P., Umesh Datta Gupta, Patel, R. B., & Owais, M. (2017). Evaluation of Aggregated Ag85B Antigen for Its Biophysical Properties, Immunogenicity, and Vaccination Potential in a Murine Model of Tuberculosis Infection. Frontiers in Immunology, 8. https://doi.org/10.3389/fimmu.2017.01608
Luo, L., Zhou, L., Luo, L., Feng, D., Ding, Y., Lu, Z., Nie, G., Bai, L., & Xiao, Y. (2023). Triamcinolone acetonide induces the autophagy of Ag85B-treated WI-38 cells via SIRT1/FOXO3 pathway. Allergologia et Immunopathologia, 51(2), 27–35. https://doi.org/10.15586/aei.v51i2.775
Prendergast, K. A., Counoupas, C., Leotta, L., Eto, C., Bitter, W., Winter, N., & Triccas, J. A. (2016). The Ag85B protein of the BCG vaccine facilitates macrophage uptake but is dispensable for protection against aerosol Mycobacterium tuberculosis infection. Vaccine, 34(23), 2608–2615. https://doi.org/10.1016/j.vaccine.2016.03.089
Murphy, B. M., & Dempsey, E. (2020). Evaluation of an Ag85B Immunosensor with Potential for Electrochemical Mycobacterium Tuberculosis Diagnostics. ECS Journal of Solid State Science and Technology, 9(11), 115011–115011. https://doi.org/10.1149/2162-8777/aba993
Anti-Mycobacterium tuberculosis Ag85B antibody [EPR28401-54] – BSA and Azide free (ab312329) | Abcam. (2025). Abcam.com. https://www.abcam.com/en-us/products/primary-antibodies/mycobacterium-tuberculosis-ag85b-antibody-epr28401-54-bsa-and-azide-free-ab312329
Waitkus, J., Chang, Y., Liu, L., Valagerahally Puttaswamy, S., Chung, T., Molina, A. M., Dollery, S. J., O’Connell, M. R., Cai, H., Tobin, G. J., Bhalla, N., & Du, K. (2022). Gold Nanoparticle Enabled Localized Surface Plasmon Resonance on Unique Gold Nanomushroom Structures for On‐Chip CRISPR‐Cas13a Sensing. Advanced Materials Interfaces, 10(1). https://doi.org/10.1002/admi.202201261
Bansal, S. A., Kumar, V., Karimi, J., Singh, A. P., & Kumar, S. (2020). Role of gold nanoparticles in advanced biomedical applications. Nanoscale Advances, 2(9), 3764–3787. https://doi.org/10.1039/d0na00472c
Gold Nanoparticles: Optical Properties – nanoComposix. (2016). NanoComposix. https://nanocomposix.com/pages/gold-nanoparticles-optical-properties?utm
Hogan, S. A., & O’Callaghan, D. J. (2010). Influence of milk proteins on the development of lactose-induced stickiness in dairy powders. International Dairy Journal, 20(3), 212–221. https://doi.org/10.1016/j.idairyj.2009.11.002
Madureira, A. R., Pereira, C. I., Gomes, A. M. P., Pintado, M. E., & Xavier Malcata, F. (2007). Bovine whey proteins – Overview on their main biological properties. Food Research International, 40(10), 1197–1211. https://doi.org/10.1016/j.foodres.2007.07.005
Khatun, S., Appidi, T., & Rengan, A. K. (2022). Casein nanoformulations – Potential biomaterials in theranostics. Food Bioscience, 50, 102200. https://doi.org/10.1016/j.fbio.2022.102200
Whey processing. (2007). Cheese Problems Solved, 163–165. https://doi.org/10.1533/9781845693534.163
CDC. (2024). Main Menu. https://www.cdc.gov/tb/webcourses/tb101/
Kolia-Diafouka, P., Godreuil, S., Bourdin, A., Carrère-Kremer, S., Kremer, L., Van de Perre, P., & Tuaillon, E. (2018). Optimized Lysis-Extraction Method Combined With IS6110-Amplification for Detection of Mycobacterium tuberculosis in Paucibacillary Sputum Specimens. Frontiers in Microbiology, 9. https://doi.org/10.3389/fmicb.2018.022
Cell Lysis Buffers – US. (n.d.). Www.thermofisher.com. https://www.thermofisher.com/us/en/home/life-science/protein-biology/protein-purification-isolation/cell-lysis-fractionation/cell-lysis-total-protein-extraction.html
Islam, M. S., Aryasomayajula, A., & Selvaganapathy, P. (2017). A review on macroscale and microscale cell lysis methods. Micromachines, 8(3), 83. https://doi.org/10.3390/mi8030083
Brinzac, M., Kuhlmann, E., Dussault, G., Ungureanu, M., Răzvan Mircea Cherecheș, & Baba, C. (2023). Defining medical deserts—an international consensus-building exercise. European Journal of Public Health, 33(5). https://doi.org/10.1093/eurpub/ckad107