Kirsten Choi and Tanishka Singh, Weston High School, Weston, MA, United States
Reviewed on 3 May 2025; Accepted on 9 June 2025; Published on 27 October 2025
With help from the 2025 BioTreks Production Team.
Lung transplants are often a life-saving intervention for patients with end-stage respiratory diseases. However, approximately 90% of lung transplants are rejected due to an aggressive immune response. Current immunosuppressant drugs, like calcineurin inhibitors (CNIs), are the standard of care for immunosuppression after lung transplantation due to their ability to lower rejection rates and improve long-term graft survival. However, they can lead to complications such as infections, increased cancer risk, and impaired tissue repair due to the widespread immune suppression, largely because these drugs are not effectively targeted and are instead administered orally or intravenously, impacting the entire immune system rather than just the transplant site. To address this, we propose a localized mRNA-based immunosuppressive strategy using lipid nanoparticle (LNP)-delivered PD-L1 mRNA. PD-L1 is a transmembrane checkpoint protein that selectively inhibits T-cell activation at the transplant site without suppressing the innate immunity systemically. The LNP formulation ensures efficient delivery of the PD-L1 mRNA into the graft tissue through both immersion and targeted injection. For the mRNA, a modified plasmid (Addgene #182263) containing the mouse PD-L1 gene, optimized for in vitro transcription and translation will be used. This targeted approach to immunosuppression is expected to reduce local inflammation while preserving the body’s overall immune system, effectively increasing graft and patient survival with fewer side effects.
Keywords: Lung transplant, Standard of care, programmed cell death-ligand 1, localized immunosuppressant, mRNA therapy
Authors are listed in alphabetical order. Mary Liu and Peter Horanyi mentored the group. Please direct all correspondence to peter.horanyi@ucb.com.


Background
Lung transplants are a critical procedure that can save the lives of patients, yet they face a significant challenge: post-transplant rejection. Approximately 90% of lung transplants are ultimately rejected by the recipient’s immune system (UT Southwestern Medical Center, 2014). This immune response is primarily driven by T-cells, which are responsible for triggering and carrying out a cascade of immune system attacks against the organ once the body recognizes the transplanted lung as foreign (Duncan & Wilkes, 2005). Around 40% of patients withlung transplants experience acute rejection, which occurs within the first year after transplantation (Mrad & Chakraborty, 2022).
To prevent rejection, the current standard of care involves administering immunosuppressant drugs to the patient (Hussain & Khan, 2022). These drugs, which include proteins and steroids, circulate in the bloodstream before being absorbed into the targeted tissue, as they are typically administered either orally or intravenously. This method of delivery is fundamentally flawed because the drugs can easily diffuse into various tissues throughout the body rather than staying localized at the transplant site. This leads to suppression of the immune system across the entire body. As a result, patients are left highly vulnerable to infections and diseases due to their weakened immune systems (McDermott & Girgis, 2018).
This highlights the need for a new approach to the standard of care for lung transplants: localized immunosuppression. This form of treatment would remain concentrated at the site of the transplant, which could significantly reduce the risk of systemic immunosuppression and address the high rate of acute rejection.
To address this issue, our research began by defining strict criteria for a potential localized immunosuppressant: it had to dampen T‑cell activity, stay near the transplant site, avoid secretion and harmful signaling, exhibit a reasonable half‑life, and be producible in vitro. We also tested IL-10 and FasL proteins, but PD‑L1 emerged as the best candidate after sequential filtering of checkpoint molecules against these criteria: checkpoint potency, membrane anchoring, localized expression, and practical delivery. As a transmembrane protein, PD-L1 is in the cell membrane of the transplanted tissue. This prevents it from diffusing into the bloodstream, effectively limiting systemic exposure. PD-L1 is also responsible for triggering the PI3K/Akt and Ras/MEK/ERK pathways, which selectively curbs T‑cell proliferation without crippling innate immunity (Han et al., 2020). To ensure the protein is expressed on‑site without repeated infusions, we chose the method of delivering lipid‑nanoparticle‑encapsulated PD‑L1 mRNA. Additionally, the PD-L1 protein’s half-life is on the hour‑scale, averaging at approximately 15 hours, which aligns with the acute‑rejection time frame(Chai et al. 2022). Administration of this drug would involve a two‑step delivery protocol: soaking the organ in PD-L1 LNPs for immediate surface coverage, then injecting the same LNP solution into the transplant tissue for deeper penetration, allowing it to incubate prior to the transplantation procedure.
The objective of this experiment is to evaluate the viability of the PD-L1 protein as a targeted and localized immunosuppressant in post-lung-transplant care in an effort to improve patient mortality and reduce acute rejection rates. We aim to determine its effectiveness by analysing its ability to reduce T-cell-mediated rejection and improve transplant success rates without significantly compromising the patient’s immune function, while also reducing the side effects.
Some possible drawbacks that may arise include challenges in the delivery of the mRNA LNPs, as the two-step delivery method (soaking and injection) may not sufficiently or uniformly distribute the mRNA LNP uptake throughout the lung. Such issues may cause partial protection, where some areas are protected while others are rejected by T-cells. A potential method to address this issue includes using fluorescent DiR dye for fluorescent labeling. By using living image software (PerkinElmer, IVIS® version: 4.7.4) to track the fluorescence in a mouse’s body, it is possible to track the location of the mRNA LNPs, both within the lung and throughout the mouse’s body, which can help us determine if the LNPs remain near the local graft tissue (Mow et al., 2024)1.
Systems Level
At the systems level, our study evaluates how localized PD-L1 delivery affects transplant tissue immunity in a whole transplant model and determines the immune response to the transplant based on the presence of the mRNA containing LNPs. The study will first be conducted in vitro testing using mouse lung epithelial cells (MLE 12 CRL-2110 ™) to test the transcription accuracy of the mouse PD-L1 plasmids in addition to seeing which transduction pathways are activated by PD-L1. Using culture dishes, coat the 100-mm tissue culture plates with 42 μg CD45 and 16 μg CD32 antibodies in 7 mL PBS for 24–48 h at 4°C, washing the plates twice with PBS and once with HEPES-buffered DMEM ( Chen & Liu, 2021). For the 3D culturing of the mouse epithelial cells, culture the cells in the Dulbecco’s Modified Eagle Medium (DMEM; Gibco) supplemented with 10% fetal bovine serum (FBS; Gibco) and 1% penicillin/streptomycin (Gibco). Afterwards, root the cells into a 6‐well culture plate at a density of 106 cells per well and culture them for 24 hours (Chen et al., 2025). Then, treat the cells with the mouse mRNA LNP to observe the fusion of the LNP to the membrane (and therefore the insertion of the mouse plasmid into the lung cell) and the transcription of the PD-L1, and evaluate the effect of the PD-L1 molecules on the cultured cells using cytotoxicity endpoints, such as lactate dehydrogenase detection and trypan blue staining. In addition to testing the mouse epithelial lung cells, it is important to test the effects of the human PD-L1 plasmids on humanoid epithelial lung cells (specifically a549 lung cells) by using a similar 3D cell culturing technique. Cell culturing would allow for the determination of dosage as well as determining the differences in the effects of the PD-L1 between mice and humans, and taking this into consideration when conducting the experiment.
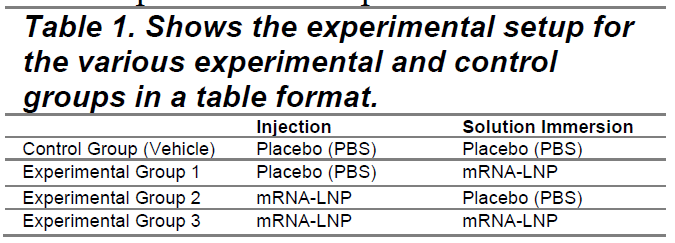
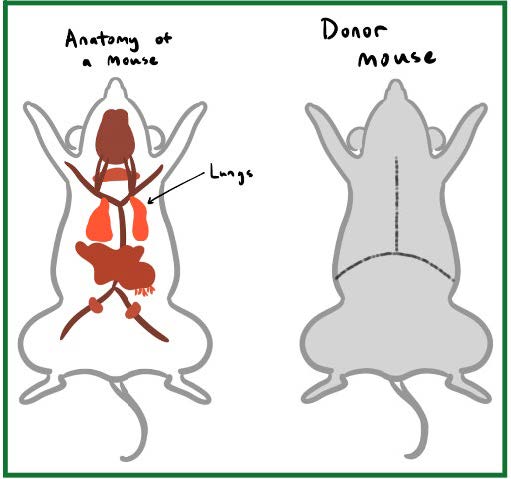
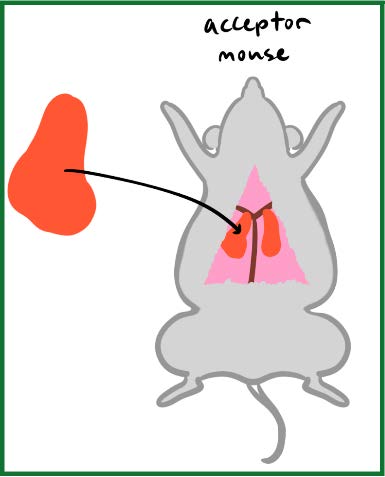
For the procedure, donor lungs are surgically extracted, briefly immersed in their assigned solution, and as mentioned, receive either the LNP or placebo injections before incubation and implantation into recipients (see Figures 1.(a), 1.(b), 1.(c)). All procedures conducted on animal subjects follow IACUC guidelines.
The independent variable in this experiment is the PD-L1 mRNA LNP solution, as found in the experimental group’s treatment composition. The dependent variable will be the presence of acute lung transplant rejection symptoms in the recipient mice. Since mice are widely used in immunology research and share many relevant immune components with humans, such as T cells, white blood cells, and CRP, blood tests such as Complete Blood Count (CBC) and C-reactive protein (CRP) will be conducted to measure immune system activity and detect potential inflammation (Mestas & Hughes, 2004). The CBC test provides a comprehensive analysis of different blood cell types, which will allow the detection of an increase in white blood cell count – a sign indicative of increased immune system activity, which aligns with acute rejection symptoms (Complete blood count (CBC): Medlineplus medical test, 2024). The CRP test measures the levels of the C-Reactive Protein released by the liver in response to inflammation, which is one of the major signs of acute rejection. Because these tests mirror standard human monitoring, they provide a realistic proxy for future clinical deployment. These diagnostic methods are also a part of the standard of care in human transplant monitoring and have also been validated in mouse models, providing a realistic and translationally relevant comparison for assessing the effectiveness of PD‑L1 treatment.
The experimental setup for the pilot test determining feasibility will consist of 3 experimental groups and a control group, with group sizes being two mice for the control and three mice each for the three experimental setups. Each group will be given a specific treatment composition to test the effectiveness of the LNP solution protein and the delivery method. The experimental groups will either receive the placebo containing a Phosphate Buffered Saline (PBS), or the actual LNP solution. The control group will receive the placebo (PBS) for both the injection and the solution immersion. Table 1 consists of an overview of the experimental setup.
|
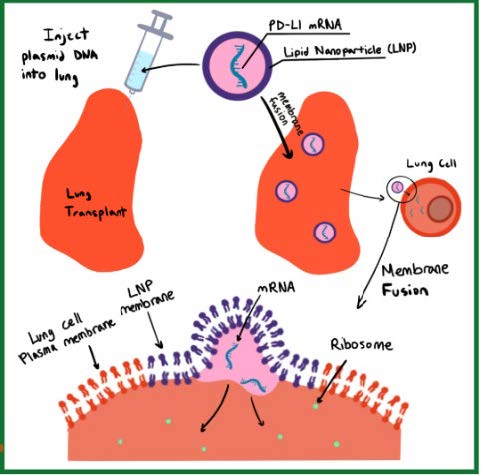
| Figure 1. (a) Shows the diagram of the donor mouse, (b) Demonstrates the transplantation, (c) Shows the LNP delivery into the lung cells. |
|
|
|
Device Level
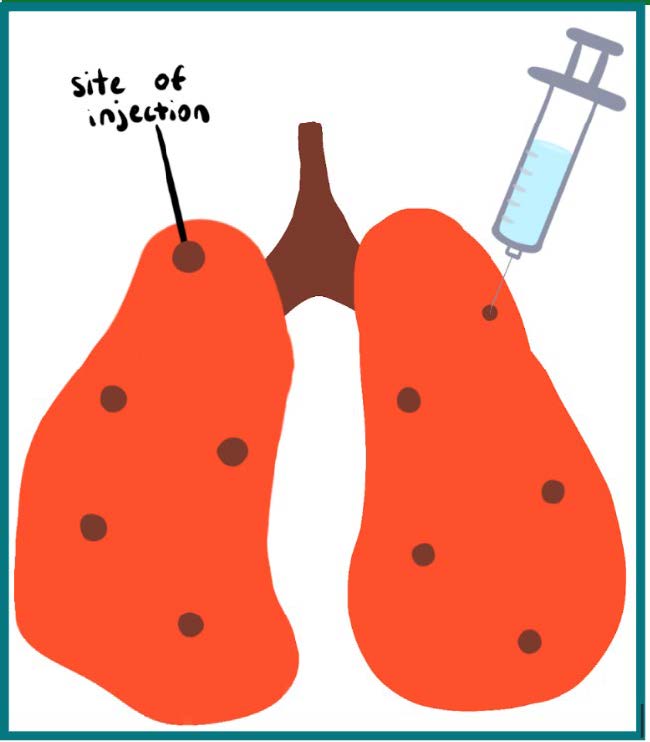
The PD-L1 protein is delivered into the lung by fully immersing the lung in a solution containing PD-L1 mRNA lipid nanoparticles (mRNA LNPs) and through direct injection of these mRNA LNPs. Injections of 20 µL will be carefully delivered into 5 distinct sites (Figure 2) across each lung to ensure an even and localized distribution of the LNP mRNA solution without causing tissue damage (Turner et al., 2011). The LNPs encapsulate the mRNA encoding PD-L1, which is then taken up by cells and translated into the functional PD-L1 protein. The resulting polypeptide is modified to stabilize the protein and ensure it functions properly, such as through glycosylation and phosphorylation.
| Figure 2. Demonstrates the injection procedure into the lungs through 5 distinct sites. |
|
This PD-L1 protein was selected due to its transmembrane characteristics and its ability to bind to the transmembrane receptor PD-1 on T-cells. Binding to the receptor activates PD-1, inducing a phosphorylation cascade that diminishes the activation signal created by the binding of T-cell antigen receptors (TCR) or CD28 to the cell transmembrane proteins on the cell. It does so by dephosphorylating key proteins, such as kinases like ZAP70 and PI3K, in the TCR transduction pathway.
The LNP will be engineered to encapsulate the PD-L1 protein mRNA and will protect the mRNA from being broken down or damaged by enzymes outside the cell. While the size of all produced LNP may not be the same, they should be around 60-100 nm. To encapsulate the mRNA into the LNP, the NanoAssembler ignite/ignite +, a microfluidic system, is used for a medium-scale production of the formula (60mL produced with a 2:1 flow rate ratio). When using the microfluidic system, two solutions must be entered into the system: the mass-produced mRNA and a lipid solution containing ionizable lipids, phospholipids, sterol lipids, and PEGylated lipids. For the optimal LNP stabilization, the solution must be made up of 0.5093 mg of ionizable lipids (ALC-0315), 0.1034 mg of PEGylated lipids {ALC-0159 [(polyethylene glycol)-2000]}, 0.4697 mg of phospholipids (DSPC), and 0.0176 mg of sterol lipids (cholesterol), all of which follow a molar N/P ratio of 6 (Schoenmaker et al., 2021). There should be 2.2 mg of PD-L1 mRNA entered into the microfluidic system. After creating the particles, dilution occurs (using the SpectraFlo Lab System) through adding a buffer to the particle solution in order to make sure that the LNP and mRNA are at optimal stability. The buffer should contain 1540 mg of potassium dihydrogen phosphate and 220 mg of disodium hydrogen phosphate dihydrate with a pH of 7–8. Afterwards, the LNPs should undergo overnight dialysis against TBS (20 mM Tris, 0.9% NaCl, pH 7.4) and should be concentrated using Amicon Ultra Centrifugal Filters with a 100 kDa molecular weight cutoff6. After the solution is concentrated, it should be stored at 4 °C before use.
Parts Level
We will use plasmid (Addgene #182263) for In Vitro Transcription (IVT) of desired PD-L1 mRNA, so that it can be incorporated into the LNPs.
It is important to change the human pDL1 (Q9NZQ7) to mouse pDL1 (Q9EP73) in this experiment as the human gene and mouse gene are only 69.2% identical(Uniprot, 2025). The plasmid will be modified using PCR-based amplification of the mouse PD-L1 gene from total mouse cDNA.
In Vitro Transcription (IVT) will be performed according to the procedure for Addgene #182263 using the kit from CellScript (kit #C-MSC100625). The protocol listed for the CellScript #C-MSC100625 is adhered to.
The details for the plasmid are as follows:
Plasmid for IVT of Desired mRNA: PD-L1 (Addgene #182263)
This plasmid is used for synthesizing single- and double-stranded RNA.
Key Features:
- Backbone Size: 2319 bp
- Promoters: T3 and SP6 for ssRNA; dual T7 promoters for dsRNA synthesis
- Bacterial Resistance: Ampicillin (100 µg/mL)
- Host Strain: DH5α, grown at 37°C
Copy Number: High - Cloning Method:
- Digest with BspQI
- Use Gibson Assembly with primers having specific overhangs:
- Forward: 5’-TTAACCCTCACTAAAGGGAG-3’
- Reverse: 5’-GGGATTTAGGTGACACTATAGAA-3’
- M13 universal primers enable full sequencing of inserts
The Steps for mRNA Production & Delivery are as follows:
There are multiple key steps in the process of mRNA production and delivery. Firstly, the desired PD-L1 gene is cloned into the plasmid (Addgene #182263). Following this step, in vitro transcription must be carried out to generate sufficient mRNA. The produced mRNA is then purified using a Qiagen kit (#28104) (Qiagen, 2024). After purification, lipid nanoparticles (LNPs) are used to encapsulate the mRNA for delivery. These LNPs will typically consist of ionizable lipids (ALC-0315), PEGylated lipids {ALC-0159, which includes polyethylene glycol-2000}, phospholipids (DSPC), and sterol lipids such as cholesterol.
Safety
Safety is prioritized in all research projects, whether it concerns the environment, ethical standards, or biological organisms. For this study, all procedures involving animal subjects will adhere to IACUC guidelines to ensure ethical research practices. Wearing full personal protective equipment (PPE) while producing the mRNA LNP is strongly recommended due to the potential exposure to toxic substances. The use of ionizable lipids (ALC-0315) is crucial to the efficiency of encapsulation; however, high exposure to these lipids can result in cytotoxicity (Bevers et al., 2022). It is imperative that all the scientists take precautions and conduct procedures with care using a biosafety cabinet in order to prevent contamination of the biological material used, in addition to maintaining environmental cleanliness.
Due to the use of live mice during the experiment, it is essential that they are treated in a humane manner and provided with necessities such as food and water, while also being handled with care. To uphold ethical research practices, we hope to reduce the number of casualties to the fullest extent by transplanting only one lung from the donor to the recipient. This can help us mitigate the risk of losing half the mouse population used in the experiment trials.
During the transplantation, it is necessary that all surgery precautions are followed, including preventing contamination, effectively monitoring anesthesia, and preserving the organ with the utmost care in order to ensure the subject has the highest chance of survival.
Finally, proper disposal of all materials is crucial to ensure environmental safety. For example, all animal carcasses should be incinerated, buried, or rendered, with incineration being the preferred method to prevent environmental contamination from any chemicals used (Protocols for Safe Handling and Disposal of Carcasses).
Discussions
Using PD-L1 mRNA LNPs to reduce T-cell activation of targeted lung cells has the potential to significantly improve the recovery of lung transplant patient. This treatment addresses the risk of lung transplant rejection and reduces the likelihood of an acute immune response by preventing apoptosis of transplant tissue cells by deactivating T-Cells in the transplant region.
Our method’s ability to localize PD-L1 protein expression allows for a more targeted approach to immunosuppressant delivery, which minimizes systemic immune suppression. Unlike traditional immunosuppressants, which are delivered intravenously or orally and require diffusion into the bloodstream to reach target tissue, our localized approach significantly reduces this risk, helping protect patients from infections and other complications that may arise from a weakened immune system.
By specifically targeting the transplant site, our method will prevent rejection in a specific region while still allowing the rest of the immune system to remain active and functional.
In addition, this study will allow the determination of the viability of a protein that could potentially save lives.
Although there are many benefits to this project, all testing and experimenting must be as thorough and accurate as possible to ensure the collected data is viable. This is because our primary goal is to eventually apply our approach to real patients, and any error could pose a serious risk to human lives. Therefore, it is imperative that we account for all potential complications. Additionally, PD-L1 is involved in multiple signal transduction pathways, beyond T-cells regulation, which poses a challenge as its expression in lung cells may trigger unintended cellular responses (Karwacz et al., 2011). This introduces uncertainty regarding potential off-target effects or adverse reactions, which need to be thoroughly investigated prior to any clinical application. To address potential off-target effects, we will monitor any side effects and identify which signaling pathways are being inadvertently activated based on these symptoms. If unintended pathways are implicated, we may reduce the dosage of PD-L1 mRNA LNPs or co-administer pathway-specific inhibitors as needed to mitigate unintended cellular responses.
Next Steps
This experiment will allow researchers to determine the viability of the PD-L1 protein in a mouse system. Depending on the results of the experiment, further research could be modified to test the protein in new conditions. Since the first round of experiments would be conducted using the mouse gene for PD-L1 (Q9EP73), the next step would be to test the human PD-L1 gene (Q9NZQ7) in the same system (Uniprot, 2025). Eventually, we want to be able to ensure that the protein is effective and safe enough to be used for human trials.
Author Contributions
K.C. and T.S. collaborated on the Abstract, Background, and Discussions sections. All images were drawn by K.C. and K.C worked on the Device Levels and Safety sections. T.S. worked on the Systems Level, Parts Level, and Next Steps sections. T.S constructed the experimental setup and table figure, collaborating with P.H.
Acknowledgements
We sincerely thank Peter Horanyi for taking the time to meet with us, for offering his insights, and for sharing his knowledge on the topic-his mentorship was invaluable to our project. We are also deeply grateful to Mary Liu for encouraging us to pursue this opportunity and for providing us with the knowledge and resources that helped bring this research to life.
References
Addgene. (n.d.). *pDL1 plasmid #182263*. Retrieved from http://n2t.net/addgene:182263
Bevers, S., Kooijmans, S. A. A., Van de Velde, E., Evers, M. J. W., Seghers, S., Gitz-Francois, J. J. J. M., van Kronenburg, N. C. H., Fens, M. H. A. M., Mastrobattista, E., Hassler, L., Sork, H., Lehto, T., Ahmed, K. E., El Andaloussi, S., Fiedler, K., Breckpot, K., Maes, M., Van Hoorick, D., Bastogne, T., & Schiffelers, R. M. (2022). mRNA-LNP vaccines tuned for systemic immunization induce strong antitumor immunity by engaging splenic immune cells. *Molecular Therapy, 30*(9), 3078–3094. https://doi.org/10.1016/j.ymthe.2022.07.007
Chai, I., Kornyeyev, D., Hsieh, E., Magombedze, G., Stapleton, L., Hung, M., Kwon, H. J., Stefanutti, E., Belzile, J. P., Czerwieniec, G., Wang, A. Y., Morar, M., & Lad, L. (2022). Effects of small molecule-induced dimerization on the programmed death ligand 1 protein life cycle. *Scientific Reports, 12*, Article 25417.
Chen, Q., & Liu, Y. (2021, January 8). Isolation and culture of mouse alveolar type II cells to study type II to type I cell differentiation. Cell press: Star protocols. https://star-protocols.cell.com/protocols/338#bib2
Chen, Y., Lin, F., Zhang, T., Xiao, Z., Chen, Y., Hua, D., Wang, Y., Wei, J., Jin, T., & Lv, X. (2025, April 5). Engineering extracellular vesicles derived from 3D cultivation of bmscs enriched with HGF ameliorate sepsis-induced lung epithelial barrier damage. Advanced science (Weinheim, Baden-Wurttemberg, Germany). https://pmc.ncbi.nlm.nih.gov/articles/PMC12021063/?utm_source=chatgpt.com
Duncan, M. D., & Wilkes, D. S. (2005). Transplant-related immunosuppression. *Proceedings of the American Thoracic Society, 2*(5), 449–455.
Epithelial cell medium – animal – Innoprot epithelial cell medium kit. Innoprot. (2024, October 17). https://innoprot.com/product/epithelial-cell-medium-animal/
Han, Y., Liu, D., & Li, L. (2020). PD-1/PD-L1 pathway: current researches in cancer. American Journal of Cancer Research, 10(3), 727. https://pmc.ncbi.nlm.nih.gov/articles/PMC7136921/
Hussain, Y., & Khan, H. (2022). Immunosuppressive drugs. In *Encyclopedia of Infection and Immunity* (Vol. 4, pp. 726–740). https://doi.org/10.1016/b978-0-12-818731-9.00068-9
Karwacz, K., Bricogne, C., MacDonald, D., Arce, F., Bennett, C. L., Collins, M., & Escors, D. (2011). PD‐L1 co‐stimulation contributes to ligand‐induced T cell receptor down‐modulation on CD8 + T cells. EMBO Molecular Medicine, 3(10), 581–592. https://doi.org/10.1002/emmm.201100165
Mestas, J., & Hughes, C. C. W. (2004). Of Mice and Not Men: Differences between Mouse and Human Immunology. The Journal of Immunology, 172(5), 2731–2738. https://doi.org/10.4049/jimmunol.172.5.2731
Mrad, A., & Chakraborty, R. K. (2022). Lung transplant rejection. In *StatPearls*. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK564391/
Mow, R. J., Srinivasan, A., Bolay, E., Merlin, D., & Yang, C. (2024, May 20). Fluorescent labeling and imaging of IL-22 mrna-loaded lipid nanoparticles. Bio-protocol. https://pmc.ncbi.nlm.nih.gov/articles/PMC11116892/#:~:text=The%20ability%20to%20track%20LNPs,in%20other%20models%20of%20interest.&text=This%20protocol%20is%20developed%20to,colitis%20sites%20using%20lipid%20nanoparticles.&text=This%20protocol%20uses%20fluorescent%20DiR,the%20gastrointestinal%20tract%20of%20mice.&text=This%20protocol%20employs%20the%20IVIS%20spectrum%20for%20imaging.
Protocols for Safe Handling and Disposal of Carcasses. CDFW. (n.d.). https://wildlife.ca.gov/Conservation/Laboratories/Wildlife-Health/Monitoring/Protocols#:~:text=Three%20common%20effective%20methods%20of,also%20be%20the%20most%20expensive.
QIAGEN. (2024). *QIAquick PCR Purification Kit*. rna-purification/dna-purification/dna-clean-up/qiaquick-pcr-purification-kit
Schoenmaker, L., Witzigmann, D., Kulkarni, J. A., Verbeke, R., Kersten, G., Jiskoot, W., & Crommelin, D. J. A. (2021, April 9). MRNA-lipid nanoparticle COVID-19 vaccines: Structure and stability. ScienceDirect. https://www.sciencedirect.com/science/article/pii/S0378517321003914
Turner, P. V., Brabb, T., Pekow, C., & Vasbinder, M. A. (2011). Administration of Substances to Laboratory Animals: Routes of Administration and Factors to Consider. Journal of the American Association for Laboratory Animal Science : JAALAS, 50(5), 600. https://pmc.ncbi.nlm.nih.gov/articles/PMC3189662/
UniProt. (2025). *UniProt Q9NZQ7 entry*.
UT Southwestern Medical Center. (2014). *Why lung transplant rejection is more normal– and treatable – than most think*. https://utswmed.org/medblog/lung-transplant-rejection/